
Importance of staying up-to-date in Research topics

It’s vital to stay current in your field of Research to ensure that your study fits into the larger context of scientific knowledge and prevent duplicating work that’s already been done. Then, because you’re expected to follow those standards, staying on top of ever-changing legal and compliance duties is a business need.

Why is it critical to keep up with the most recent Research?
There are several reasons why it’s critical to stay current with your field of study changes.
Identifying fresh Research opportunities
Understanding the present state of knowledge on a topic, recognizing gaps, and focusing on a meaningful and responsive issue. A thorough literature search can help you find a research topic that is precise enough to be examined in the context of a specific test.
Also, to ensure that you don’t leave any important studies out of your literature review, staying current will assist you in defining your long-term research goals and career trajectory, not just the next topic to concentrate on.
The findings of the Research have an expiration date.
Time is a critical factor in the systematic review process and an important covariate in assessing study heterogeneity and a fundamental determinant of systematic review clinical relevance. Indeed, systematic reviews’ usefulness as a foundation for evidence-based practice depends on proper time considerations.
New Research-based on Previous works
Previous work can help you figure out which methodologies to utilize, what data or resources are already freely available to work with, and what Research limits to solve. Developing beneficial relationships with potential collaborators
As Research entails testing, verifying, and rejecting hypotheses regularly, keeping up with recent publications will assist you in defining building blocks for your study.
Guidance & Confirming that your Research is focused on a new topic
One of the key responsibilities for a doctorate adviser, department head, or field expertise is to advise students on relevant research subjects.
Staying current on literature in your line of work and learning how to do it effectively will help you better support them and guide their research careers. You will not only be assisting them in their career advancements, but you will also be contributing to the improvement of your discipline as a whole.
Observing what your competitors are doing
Research involves many activities. As a researcher, you rely on the information and insights of other researchers to help you understand specific elements of your profession or related disciplines.
How do I stay current with Research Topics?
Keeping upto date may appear daunting at first, but your sources can be divided into two categories: formal and informal. You’ll need to put up mechanisms for the many sources you deem to be relevant if you want to stay on top of newly published and emergent Research .
As your priorities may alter over time, you’ll need to go back and evaluate your notifications from time to time, especially if you’re performing your Research over several months or even years. To track changes in the direction of your original study interest, you have to create new alerts. As a result, keeping up with the Research Topics can help you uncover potential solutions or alternatives to problems you’re having with your study.
Related Posts
Interrogative pronoun – english editing..
The interrogative pronouns are : Who, whom, whose, what, which. They are used in the formation of questions: What is homeopathy? For Scientific english editing and Medical Writing Services visitwww.manuscriptedit.com
Superlative – English editing.
Many adjectives can have three forms: Absolute Comparative Superlative Small smaller smallest Attractive more attractive most attractive The comparative form is used when comparing two items; the superlative is used when there are more than two: She is smaller than her brother. (comparative) The smallest of the three specialist colleges, it has just over 150 […]
Intensifier – English editing.
An adverb that is used to modify an adjective. Intensifiers show how much of a quality something has. For example: A beautiful view. A rather beautiful tropical garden. Extremely beautiful drawings. Intensifiers can also modify other adverbs. For example: Easily Fairly easily Incredibly easily. For Scientific english editing and Medical Writing Services visitwww.manuscriptedit.com
Leave a Reply Cancel reply
Your email address will not be published. Required fields are marked *
Save my name, email, and website in this browser for the next time I comment.
- U.S. Department of Health & Human Services
- Virtual Tour
- Staff Directory
- En Español
You are here
Science, health, and public trust.
September 8, 2021
Explaining How Research Works

We’ve heard “follow the science” a lot during the pandemic. But it seems science has taken us on a long and winding road filled with twists and turns, even changing directions at times. That’s led some people to feel they can’t trust science. But when what we know changes, it often means science is working.

Explaining the scientific process may be one way that science communicators can help maintain public trust in science. Placing research in the bigger context of its field and where it fits into the scientific process can help people better understand and interpret new findings as they emerge. A single study usually uncovers only a piece of a larger puzzle.
Questions about how the world works are often investigated on many different levels. For example, scientists can look at the different atoms in a molecule, cells in a tissue, or how different tissues or systems affect each other. Researchers often must choose one or a finite number of ways to investigate a question. It can take many different studies using different approaches to start piecing the whole picture together.
Sometimes it might seem like research results contradict each other. But often, studies are just looking at different aspects of the same problem. Researchers can also investigate a question using different techniques or timeframes. That may lead them to arrive at different conclusions from the same data.
Using the data available at the time of their study, scientists develop different explanations, or models. New information may mean that a novel model needs to be developed to account for it. The models that prevail are those that can withstand the test of time and incorporate new information. Science is a constantly evolving and self-correcting process.
Scientists gain more confidence about a model through the scientific process. They replicate each other’s work. They present at conferences. And papers undergo peer review, in which experts in the field review the work before it can be published in scientific journals. This helps ensure that the study is up to current scientific standards and maintains a level of integrity. Peer reviewers may find problems with the experiments or think different experiments are needed to justify the conclusions. They might even offer new ways to interpret the data.
It’s important for science communicators to consider which stage a study is at in the scientific process when deciding whether to cover it. Some studies are posted on preprint servers for other scientists to start weighing in on and haven’t yet been fully vetted. Results that haven't yet been subjected to scientific scrutiny should be reported on with care and context to avoid confusion or frustration from readers.
We’ve developed a one-page guide, "How Research Works: Understanding the Process of Science" to help communicators put the process of science into perspective. We hope it can serve as a useful resource to help explain why science changes—and why it’s important to expect that change. Please take a look and share your thoughts with us by sending an email to [email protected].
Below are some additional resources:
- Discoveries in Basic Science: A Perfectly Imperfect Process
- When Clinical Research Is in the News
- What is Basic Science and Why is it Important?
- What is a Research Organism?
- What Are Clinical Trials and Studies?
- Basic Research – Digital Media Kit
- Decoding Science: How Does Science Know What It Knows? (NAS)
- Can Science Help People Make Decisions ? (NAS)
Connect with Us
- More Social Media from NIH
How recent is recent for good referencing?

Cited articles (i.e., references) in a research paper play a central role in demonstrating the necessity of the research and establishing the validity and significance of the research results.
Therefore, good referencing practices (e.g., citing relevant, critical, and recent research works on the topics) not only increase the quality of the research paper but also facilitate its peer review and availability to the right audience.
Citing or referencing recent articles in the research paper assures reviewers that an extensive literature review was undertaken while writing the paper and information in the paper is up to date. This builds trust between the authors of the paper and the reviewers, which may influence peer review reports.
How old is gold?
All being said, do we exactly know how old a research article can be before it gets the label of not being recent i.e., an old article not good for citing.
There is consensus among scientists and researchers that articles less than five years old are recent publications. However, it may vary from discipline to discipline. For example, researchers in fast-moving fields (e.g., nanotechnology or artificial intelligence) may feel 5-years is too old whereas those in biology may not have the same feeling.
How many recent references make a research paper contemporaneous?
Santini et al. (20018) suggested that if the most recent reference is more than 5 years or so, it can indicate that a full up to date review of the literature has not been undertaken.
However, the suggestion is a weak indicator of the comprehensiveness of the literature review done while writing a paper as it is based on the measure of only one reference.
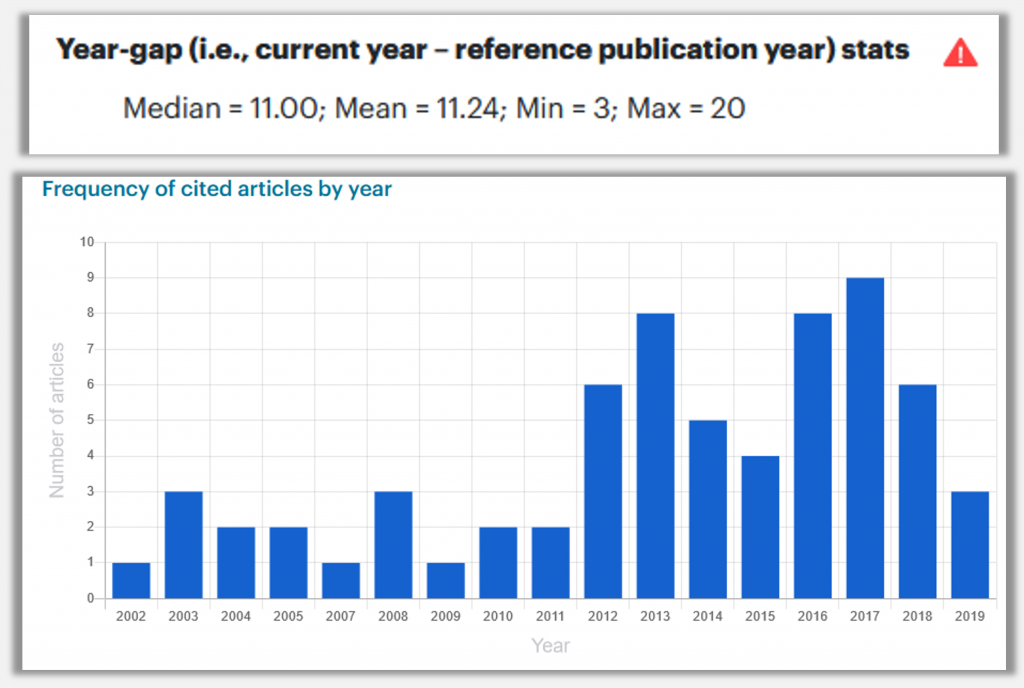
To build a robust understanding of the matter, nXr team analyzed how old references of 69 research papers (published in three highly acclaimed journals: Nature, Science, and Cell) were.

The graph clearly shows that 50% of references in the articles published in highly acclaimed journals are less than 6 years old. This indicates that well-written articles have the characteristic to cite more recent research papers.
How to get similar information for the references in the research paper you are writing?
No worries! When you cite using nXr reference manager and citation tool , nXr automatically creates a dashboard (accessible from your nXr.iLibrary) for the references in your research paper containing various data visualizations.
In one such visualization, you can see the publication year distribution of the references (see below). nXr also gives you an alert if 50% of the references are more than 5 years old so that you can check them.
Stack Exchange Network
Stack Exchange network consists of 183 Q&A communities including Stack Overflow , the largest, most trusted online community for developers to learn, share their knowledge, and build their careers.
Q&A for work
Connect and share knowledge within a single location that is structured and easy to search.
When is it appropriate to describe research as "recent"?
I want to write: "A recent study ..." ,
The particular study I want to cite was published two years ago. I don't think that this is very recent in terms of journal appearances. But it is the most recent I could find compared to similar studies, which is what I want to emphasize.
But what are the general semantics of "recent" when referencing sources?
- 10 If the date of the study matters, why not "A study from 2014...."? – mdd Commented Mar 9, 2016 at 0:44
- 8 It is an ineffective way of saying "This is important!" As a reviewer I would probably tolerate descriptions of anything from the past ten years as "recent." – Anonymous Physicist Commented Mar 9, 2016 at 1:32
- 3 In my mind recent is anything that is new enough that it hasn't been fully absorbed (worked its way into later research, publications and into people's minds). That might depend on recent to whom -- a 20 year-old mathematical theory might well be too recent to have fully worked its way into engineering practice, so if you're writing to the engineering audience it could be appropriate to call it recent. – Owen Commented Mar 9, 2016 at 3:40
- 4 Redundancy is not a bad thing in academic writing. – Dirk Commented Mar 9, 2016 at 5:23
- 4 Keep in mind that recent to you may not be recent to a future reader. If you have something more specific to convey ("most recent at the time of writing", "unsettled", "currently the hip and trendy thing that gets grants"), you'd be best served being more specific. Otherwise, your reader will have to look at your paper's publication date and try to work out what you meant from context. – Jeffrey Bosboom Commented Mar 9, 2016 at 10:26
4 Answers 4
Good question. The semantics of the word "recent", in general, and in academic writing, in particular, is not clearly defined (that is, fuzzy), which makes its practical use quite tricky, as evidenced by your question.
While @vonbrand's answer offers some valuable insights, such as considering the fluidity of a particular scientific field or domain, I would suggest a more practical solution to this problem, as follows. Consider literature that you reference in a particular paper. What is the temporal range of the sources? I think that this aspect could guide you in to where the word "recent" is appropriate and where not so much.
For example, if you cite sources from the current century as well as 1930s, then a paper from 2010 should be considered recent, but not one from 1950. If, on the other hand, your temporal range of references is rather narrow, say, recent 20 years, then you should refer to as "recent" for sources that are from approximately last 4-5 years. You can come up with your own rule of thumb (10-20% of the total range sounds pretty reasonable). The most important aspect would be not the actual value (for the rule of thumb), but rather your consistency in applying it throughout the paper.
- @thrau: My pleasure! Thank you for kind words and accepting. – Aleksandr Blekh Commented Mar 10, 2016 at 20:45
It depends on the area. If you are talking about slow moving areas, "recent" could be a decade ago; for something that moves fast, what was published last year is old hat.
Perhaps the easiest way out is to be more specific, "a study three years back..." (besides, the study might be several years back, or be a decade long study, but the journal issue just came out, so the publication date isn't necessarily telling).
As previously mentioned, the meaning of 'recent' depends on the topic of study. What is considered recent in mathematics may not be considered recent enough for computer science. My computer science professors have generally stuck with anything five years old as being the 'oldest' an article can be. Two to three years is generally better, especially in the tech field as things progress at a much higher rate. A good thing to look out for is when an article might pass the 5 year mark, someone will most likely have adapted the methodology or research findings in a more recent article. Best of luck!
It depends.
If you refer to something that has a precise date, you should be precise. I see no advantage in writing "A recent study showed..." over "The study X from 2010 showed..." The latter contains more information and reads as least as good (in my opinion even better, because it's more precise). A similar case is "The problem posed by X at the meeting Y in 2010..." (better than "The recently posed problem...").
One case in which "recent" could make sense is "The field X has attracted much attention recently" because usually one can not pin down an exact date for this event. However, in most cases this reads more like a self-perpetuating empty statement (if there is a simple reason why the reader should care about the field X then give that!). I have to admit that I myself also wrote sentences like this, but looking back it reads a bit weird. Nowadays, if I read "this field has attracted much attention recently" I really read that the authors do not know a good reason why their problem is interesting but feel that they should.
- On a slightly related note, how would you feel about "This field has attracted much attention recently because reasons "? – svavil Commented Mar 9, 2016 at 22:40
- I would say, the more precise the better. Probably in such a sentence just giving the reason that you feel that make the field exciting is enough. The additional information that these exciting facts resulted in "much attention recently" seems not so important. I would find it even better if the sentence would tell that the field is relevant and not that its fancy right now. – Dirk Commented Mar 10, 2016 at 10:51
You must log in to answer this question.
Not the answer you're looking for browse other questions tagged citations ..
- Featured on Meta
- Announcing a change to the data-dump process
- Upcoming initiatives on Stack Overflow and across the Stack Exchange network...
- We spent a sprint addressing your requests — here’s how it went
Hot Network Questions
- How to request for a package to be added to the Fedora repositories?
- Could today's flash memory be used instead of RAM in 1980s 8 bit machines?
- The book where someone can serve a sentence in advance
- How do cables and cooling lines transverse the pressure hull of the International Space Station?
- Can loops/cycles (in a temporal sense) exist without beginnings?
- Introducing a fixed number of random substitutions in a sequence
- Is increasing Average Product(AP) always implying increasing Marginal Product(MP) in microeconomics?
- What was the Night in Genesis 1?
- How should I run cable across a steel beam?
- Why does "They be naked" use the base form of "be"?
- How could double damage be explained in-universe?
- Jellium Hamiltonian in the thermodynamic limit
- What are the ways compilers recognize complex patterns?
- Holding *west* on the 090 radial?
- Purpose of Green/Orange switch on old flash unit
- Parking ticket for parking in a private lot reserved for customers of X, Y, and Z business's
- Why do protocol developers work on maximizing miner revenue?
- How can a Warlock learn Magic Missile?
- How can I insert new arguments to this block of function calls that follow a pattern?
- Domestic Air Travel within the US with Limited Term Driver's License and no passport, for non-resident aliens?
- How could warfare be kept using pike and shot like tactics for 700 years?
- How accurate does the ISS's velocity and altitude need to be to maintain orbit?
- Welch t-test p-values are poorly calibrated for N=2 samples
- Was supposed to be co-signer on auto for daughter but I’m listed the buyer
More From Forbes
The role of research at universities: why it matters.
- Share to Facebook
- Share to Twitter
- Share to Linkedin
(Photo by William B. Plowman/Getty Images)
Teaching and learning, research and discovery, synthesis and creativity, understanding and engagement, service and outreach. There are many “core elements” to the mission of a great university. Teaching would seem the most obvious, but for those outside of the university, “research” (taken to include scientific research, scholarship more broadly, as well as creative activity) may be the least well understood. This creates misunderstanding of how universities invest resources, especially those deriving from undergraduate tuition and state (or other public) support, and the misperception that those resources are being diverted away from what is believed should be the core (and sole) focus, teaching. This has led to a loss of trust, confidence, and willingness to continue to invest or otherwise support (especially our public) universities.
Why are universities engaged in the conduct of research? Who pays? Who benefits? And why does it all matter? Good questions. Let’s get to some straightforward answers. Because the academic research enterprise really is not that difficult to explain, and its impacts are profound.
So let’s demystify university-based research. And in doing so, hopefully we can begin building both better understanding and a better relationship between the public and higher education, both of which are essential to the future of US higher education.
Why are universities engaged in the conduct of research?
Universities engage in research as part of their missions around learning and discovery. This, in turn, contributes directly and indirectly to their primary mission of teaching. Universities and many colleges (the exception being those dedicated exclusively to undergraduate teaching) have as part of their mission the pursuit of scholarship. This can come in the form of fundamental or applied research (both are most common in the STEM fields, broadly defined), research-based scholarship or what often is called “scholarly activity” (most common in the social sciences and humanities), or creative activity (most common in the arts). Increasingly, these simple categorizations are being blurred, for all good reasons and to the good of the discovery of new knowledge and greater understanding of complex (transdisciplinary) challenges and the creation of increasingly interrelated fields needed to address them.
It goes without saying that the advancement of knowledge (discovery, innovation, creation) is essential to any civilization. Our nation’s research universities represent some of the most concentrated communities of scholars, facilities, and collective expertise engaged in these activities. But more importantly, this is where higher education is delivered, where students develop breadth and depth of knowledge in foundational and advanced subjects, where the skills for knowledge acquisition and understanding (including contextualization, interpretation, and inference) are honed, and where students are educated, trained, and otherwise prepared for successful careers. Part of that training and preparation derives from exposure to faculty who are engaged at the leading-edge of their fields, through their research and scholarly work. The best faculty, the teacher-scholars, seamlessly weave their teaching and research efforts together, to their mutual benefit, and in a way that excites and engages their students. In this way, the next generation of scholars (academic or otherwise) is trained, research and discovery continue to advance inter-generationally, and the cycle is perpetuated.
Best High-Yield Savings Accounts Of 2024
Best 5% interest savings accounts of 2024.
University research can be expensive, particularly in laboratory-intensive fields. But the responsibility for much (indeed most) of the cost of conducting research falls to the faculty member. Faculty who are engaged in research write grants for funding (e.g., from federal and state agencies, foundations, and private companies) to support their work and the work of their students and staff. In some cases, the universities do need to invest heavily in equipment, facilities, and personnel to support select research activities. But they do so judiciously, with an eye toward both their mission, their strategic priorities, and their available resources.
Medical research, and medical education more broadly, is expensive and often requires substantial institutional investment beyond what can be covered by clinical operations or externally funded research. But universities with medical schools/medical centers have determined that the value to their educational and training missions as well as to their communities justifies the investment. And most would agree that university-based medical centers are of significant value to their communities, often providing best-in-class treatment and care in midsize and smaller communities at a level more often seen in larger metropolitan areas.
Research in the STEM fields (broadly defined) can also be expensive. Scientific (including medical) and engineering research often involves specialized facilities or pieces of equipment, advanced computing capabilities, materials requiring controlled handling and storage, and so forth. But much of this work is funded, in large part, by federal agencies such as the National Science Foundation, National Institutes of Health, US Department of Energy, US Department of Agriculture, and many others.
Research in the social sciences is often (not always) less expensive, requiring smaller amount of grant funding. As mentioned previously, however, it is now becoming common to have physical, natural, and social scientist teams pursuing large grant funding. This is an exciting and very promising trend for many reasons, not the least of which is the nature of the complex problems being studied.
Research in the arts and humanities typically requires the least amount of funding as it rarely requires the expensive items listed previously. Funding from such organizations as the National Endowment for the Arts, National Endowment for the Humanities, and private foundations may be able to support significant scholarship and creation of new knowledge or works through much more modest grants than would be required in the natural or physical sciences, for example.
Philanthropy may also be directed toward the support of research and scholarly activity at universities. Support from individual donors, family foundations, private or corporate foundations may be directed to support students, faculty, labs or other facilities, research programs, galleries, centers, and institutes.
Who benefits?
Students, both undergraduate and graduate, benefit from studying in an environment rich with research and discovery. Besides what the faculty can bring back to the classroom, there are opportunities to engage with faculty as part of their research teams and even conduct independent research under their supervision, often for credit. There are opportunities to learn about and learn on state-of-the-art equipment, in state-of-the-art laboratories, and from those working on the leading edge in a discipline. There are opportunities to co-author, present at conferences, make important connections, and explore post-graduate pathways.
The broader university benefits from active research programs. Research on timely and important topics attracts attention, which in turn leads to greater institutional visibility and reputation. As a university becomes known for its research in certain fields, they become magnets for students, faculty, grants, media coverage, and even philanthropy. Strength in research helps to define a university’s “brand” in the national and international marketplace, impacting everything from student recruitment, to faculty retention, to attracting new investments.
The community, region, and state benefits from the research activity of the university. This is especially true for public research universities. Research also contributes directly to economic development, clinical, commercial, and business opportunities. Resources brought into the university through grants and contracts support faculty, staff, and student salaries, often adding additional jobs, contributing directly to the tax base. Research universities, through their expertise, reputation, and facilities, can attract new businesses into their communities or states. They can also launch and incubate startup companies, or license and sell their technologies to other companies. Research universities often host meeting and conferences which creates revenue for local hotels, restaurants, event centers, and more. And as mentioned previously, university medical centers provide high-quality medical care, often in midsize communities that wouldn’t otherwise have such outstanding services and state-of-the-art facilities.
(Photo by Justin Sullivan/Getty Images)
And finally, why does this all matter?
Research is essential to advancing society, strengthening the economy, driving innovation, and addressing the vexing and challenging problems we face as a people, place, and planet. It’s through research, scholarship, and discovery that we learn about our history and ourselves, understand the present context in which we live, and plan for and secure our future.
Research universities are vibrant, exciting, and inspiring places to learn and to work. They offer opportunities for students that few other institutions can match – whether small liberal arts colleges, mid-size teaching universities, or community colleges – and while not right for every learner or every educator, they are right for many, if not most. The advantages simply cannot be ignored. Neither can the importance or the need for these institutions. They need not be for everyone, and everyone need not find their way to study or work at our research universities, and we stipulate that there are many outstanding options to meet and support different learning styles and provide different environments for teaching and learning. But it’s critically important that we continue to support, protect, and respect research universities for all they do for their students, their communities and states, our standing in the global scientific community, our economy, and our nation.

- Editorial Standards
- Reprints & Permissions
Join The Conversation
One Community. Many Voices. Create a free account to share your thoughts.
Forbes Community Guidelines
Our community is about connecting people through open and thoughtful conversations. We want our readers to share their views and exchange ideas and facts in a safe space.
In order to do so, please follow the posting rules in our site's Terms of Service. We've summarized some of those key rules below. Simply put, keep it civil.
Your post will be rejected if we notice that it seems to contain:
- False or intentionally out-of-context or misleading information
- Insults, profanity, incoherent, obscene or inflammatory language or threats of any kind
- Attacks on the identity of other commenters or the article's author
- Content that otherwise violates our site's terms.
User accounts will be blocked if we notice or believe that users are engaged in:
- Continuous attempts to re-post comments that have been previously moderated/rejected
- Racist, sexist, homophobic or other discriminatory comments
- Attempts or tactics that put the site security at risk
- Actions that otherwise violate our site's terms.
So, how can you be a power user?
- Stay on topic and share your insights
- Feel free to be clear and thoughtful to get your point across
- ‘Like’ or ‘Dislike’ to show your point of view.
- Protect your community.
- Use the report tool to alert us when someone breaks the rules.
Thanks for reading our community guidelines. Please read the full list of posting rules found in our site's Terms of Service.
When is the evidence too old?
A few weeks ago, when submitting an abstract to a nursing conference, I was suddenly faced with a dilemma about age. Not my own age, but the age of evidence I was using to support my work. One key element of the submission criteria was to provide five research citations to support the abstract, and all citations were to be less than ten years old. This requirement left me stumped for a while. The research I wanted to cite was more than ten years old, yet it was excellent research within a very small body of work on the topic. Suddenly I struggled to meet the criteria and almost gave up on the submission, thinking my abstract would not tick all of the boxes if I used research now deemed to be ‘out of date’. I suddenly thought about all of the work I had published more than ten years ago – all that hard work past its use-by date.
Way back in the mid 1990s, a colleague and I started to have conversations with Australian nurses about the importance of evidence based practice (EBP) for the future of Australian nursing. The movement away from the comfort of ‘ritual and routine’ to the uncertainty of EBP was challenging. At the time we described EBP according to the principle that “all interventions should be based on the best currently available scientific evidence” 1 . We had embraced the ideas of authors such as Ian Chalmers 2 and were keen to educate nurses and nursing students about “practices that had been clearly shown to work and question practices for which no evidence exists and discard those which have been shown to do harm” 1 It was very much about the importance of using the most ‘robust’ and ‘reliable’ evidence that we had available to guide us in clinical decision making, taking into account individual patients at the centre of care. It was also about teaching nurses and nursing students about how to ask the right questions, where to look for answers and how to recognize when you have found the right answer to support individualized patient care.
Definitions of evidence-based practice are quite varied and I have heard nurses talk about using “current best evidence” while others use the “most current evidence”. These are quite different approaches, with the latter statement suggesting that more recent is best. This is sometimes reinforced in nursing education, where students are graded according to the use of recent research, with limitations placed on the age of resources used to support their work. However, I wonder if we are losing something in this translation about the meaning of ‘best evidence’ to support care. When does the published evidence get too old and where do we draw the line and stop reading research from our past?
Personally I have always expected my students to use up to date research when supporting their recommendations for care. However, I have also encouraged them to look back to see where the new research has come from and to acknowledge the foundation it has been built on. I am always keen to hear about the latest developments in healthcare and work to support the readers of EBN who need and want to know about what is new and important in the health care literature. Keeping up to date with new evidence is critically important for change. But I wonder how we strike a balance between absorbing recent research and taking into account robust research that preceded its publication by more than a decade?
So, let’s think about these ideas for a minute. If we put our blinkers on and ignore important research from the recently ‘outdated’ literature from the 1990s (when I first became interested in doing research), we could miss some important foundational work that still influences practice today. The two references I have used below, both from the 1990s, would not be included in the discussion at all. If we only consider literature that is recent, and value that more highly than if it is robust, then we will be missing important evidence to inform practice. Researchers could start asking the same research questions over and over (I have seen some of this already in nursing literature) and even feel pressured to repeat previous studies all over again to check if the findings still hold true in the contemporary world. Perhaps that is something to watch for in the future.
It is important to keep up to date with current research findings, new innovations in care, recent trends in patient problems, trends in patient outcomes and changes in the social, political and system context of the care we provide. But it is also important to look back as we move forward, thinking about the strength of the evidence as well as its age.
Allison Shorten RN RM PhD
Yale University School of Nursing
References:
- Shorten A. & Wallace MC. ‘Evidence-based practice – The future is clear’. Australian Nurses Journal, 1996, Vol. 4, No. 6, pp. 22-24.
- Chalmers I. The Cochrane collaboration: Preparing, maintaining, and disseminating systematic reviews of the effects of health care, Annals New York Academy of Science, 1993, Vol. 703, pp. 156-165.
Comment and Opinion | Open Debate
The views and opinions expressed on this site are solely those of the original authors. They do not necessarily represent the views of BMJ and should not be used to replace medical advice. Please see our full website terms and conditions .
All BMJ blog posts are posted under a CC-BY-NC licence
BMJ Journals
The “outdated sources” myth

- In-Text Citations
- Reference List
- Research and Publication

In this series, we will look at common APA Style misconceptions and debunk these myths one by one.
We often receive questions about whether sources must have been published within a certain time frame to be cited in a scholarly paper. Many writers incorrectly believe in the “outdated sources” myth, which is that sources must have been published recently, such as the last 5 to 10 years.
However, there is no timeliness requirement in APA Style guidelines (as defined in the Concise Guide to APA Style, Seventh Edition and Publication Manual of the American Psychological Association, Seventh Edition ). Properly citing relevant sources is a key task for writers of any APA Style paper. You should “cite the work of those individuals whose ideas, theories, or research have directly influenced your work. The works you cite provide key background information, support or dispute your thesis, or offer critical definitions and data” (American Psychological Association, 2020, p. 253). We recommend citing reliable, primary sources with the most current information whenever possible.
What it means to be “timely” varies across fields or disciplines. Seminal research articles and/or foundational books can remain relevant for a long time and help establish the context for a given paper. For example, Albert Bandura’s Bobo doll experiment (Bandura et al., 1961) is often cited in contemporary social and child psychology articles. Remember, APA Style has no year-related cutoff.
As always, defer to your instructor’s guidelines when writing student papers. For example, your instructor may require sources be published within a certain timeframe for student papers. If so, follow that guideline for work in that class. Similarly, consider the discipline and audience for whom you are writing. For example, if you are submitting an article to a journal in a fast-developing field like neuroscience, more recent sources—if relevant and important for your readers to consider in the context of your paper—might make your article more competitive.
Now that we’ve debunked another myth, go forth APA Style writers, and cite noteworthy and relevant sources!
What myth should we debunk next? Leave a comment below.
American Psychological Association. (2020). Publication Manual of the American Psychological Association (7th ed.). https://doi.org/10.1037/0000165-000
Bandura, A., Ross, D., & Ross, S. A. (1961). Transmission of aggression through imitation of aggressive models. Journal of Abnormal and Social Psychology , 63 (3), 575–582. https://doi.org/10.1037/h0045925
Related and recent
Comments are disabled due to your privacy settings. To re-enable, please adjust your cookie preferences.
APA Style Monthly
Subscribe to the APA Style Monthly newsletter to get tips, updates, and resources delivered directly to your inbox.
Welcome! Thank you for subscribing.
APA Style Guidelines
Browse APA Style writing guidelines by category
- Abbreviations
- Bias-Free Language
- Capitalization
- Italics and Quotation Marks
- Paper Format
- Punctuation
- Spelling and Hyphenation
- Tables and Figures
Full index of topics
Cookies on the NHS England website
We’ve put some small files called cookies on your device to make our site work.
We’d also like to use analytics cookies. These send information about how our site is used to a service called Google Analytics. We use this information to improve our site.
Let us know if this is OK. We’ll use a cookie to save your choice. You can read more about our cookies before you choose.
Change my preferences I'm OK with analytics cookies
Maximising the benefits of research: Guidance for integrated care systems
England has a vibrant research and development ecosystem, with well-developed research infrastructure and research expertise within our health and care workforce. The value of research in transforming health and care is significant; additionally, staff satisfaction, recruitment and retention is higher among staff who are involved in research. The inception of integrated care systems (ICSs) provides the opportunity for systems to embed research within health and care for the benefit of our population. Supporting this opportunity, a clear research thread runs through ICS strategies and plans, from joint strategic needs assessments and joint health and wellbeing strategies , integrated care strategies , joint forwards plans , integrated care board (ICB) annual reports and the assessment by NHS England of the discharge of duties by ICBs.
The Health and Care Act 2022 (the 2022 Act) sets new legal duties on ICBs around the facilitation and promotion of research in matters relevant to the health service, and the use in the health service of evidence obtained from research. NHS England will assess ICBs for their discharge of these duties. The ICS design framework sets the expectation that in arranging provision of health services, ICBs will facilitate their partners in the health and care system to work together, combining expertise and resources to foster and deploy research and innovations. This guidance supports ICBs in fulfilling their research duties.
ICSs are encouraged to develop a research strategy that aligns to or could be included in their integrated care strategy. This strategy will enable the unification of research across ICS partners, and be consistently embedded to:
- identify and address local research priorities and needs, and work collaboratively to address national research priorities
- improve the quality of health and care and outcomes for all through the evidence generated by research
- increase the quality, quantity and breadth of research undertaken locally
- extend and expand research in settings such as primary care, community care, mental health services, public health and social care
- drive the use of research evidence for quality improvement and evidence-based practice
- influence the national research agenda to better meet local priorities and needs
- improve co-ordination and standardisation within and between localities for the set up and delivery of research
- harness the patient and economic benefits of commercial contract research
- co-ordinate and develop the research workforce across all settings.
1. Introduction
This guidance sets out what good research practice looks like. It supports integrated care systems (ICSs) to maximise the value of their duties around research for the benefit of their population’s health and care and, through co-ordination across ICSs, for national and international impact. It supports integrated care boards (ICBs), integrated care partnerships (ICPs) and their partners to develop a research strategy that aligns to or can be incorporated into their integrated care strategy, and helps them and their workforce to build on existing research initiatives and activities across health and social care to improve sector-wide performance and best practice
- explains the ICB legal duties and other requirements around research and the use of evidence from research, and that research is included in forward planning and reporting
- encourages system leaders to develop a footprint-wide research strategy that aligns to local and national research priorities, develops and supports their workforce, takes the opportunities offered by commercial research and includes plans to embed research in their system’s governance and leadership
- identifies best practice examples and other resources that ICBs may find useful as they develop their research strategies.
This guidance provides comprehensive information for use by:
- those with senior responsibility, including at board level, for research strategy development and/or operationalising research
- managers responsible for developing joint strategic needs assessments, integrated care strategies, joint health and wellbeing strategies, joint forward plans, other linked strategies, or reporting on ICB activities
- research managers
- research and development/innovation leads
- heads of services
- knowledge and library specialists.
It may also be useful to individuals involved in research, education, and partner organisations such as local authorities, social care services, the voluntary, community and social enterprise sector (VCSE) and other providers of healthcare services.
NHS England provides guidance on embedding research in the NHS and secure data environments, and the Office for Life Sciences (OLS ) champions research, innovation and the use of technology to transform health and care service. Other sources of guidance, support and information are signposted in this guidance to support ICSs in aligning to national visions, strategies and plans around research.
1.1 Definition of research
NHS England uses the UK Policy Framework for Health and Social Care Research definition of research:
“… the attempt to derive generalisable or transferable new knowledge to answer or refine relevant questions with scientifically sound methods. This excludes audits of practice and service evaluation. It includes activities that are carried out in preparation for or as a consequence of the interventional part of the research, such as screening potential participants for eligibility, obtaining participants’ consent and publishing results. It also includes non-interventional health and social care research (that is, projects that do not involve any change in standard treatment, care, or other services), projects that aim to generate hypotheses, methodological research and descriptive research”.
This broad definition encompasses the range of types of research:
- clinical trials and other clinical investigations into the safety and effectiveness of medicines, devices and health technologies
- public health research
- observational studies
- discovery science and experimental medicine
- translational research in which results from basic research are developed into results that directly benefit people
- applied research
- research to support policy-making and commissioning
- social care research and research in social care settings
- research into NHS services and care pathways.
1.2 Why research is important
The UK is a world leader for research and invention in healthcare, with around 25% of the world’s top 100 prescription medicines being discovered and developed in the UK ( The impact of collaboration: The value of UK medical research to EU science and health ). Research in the health and care system is important because it underpins all advances in health and care and is the basis for evidence-based practice. Engaging clinicians and healthcare organisations in research is associated with improvements in delivery of healthcare ( Does the engagement of clinicians and organisations in research improve healthcare performance: a three-stage review) . To benefit service users and the public, the NHS and local government, and achieve return on investment, it is vital that research is disseminated, shared and translated into practice.
The National Institute for Health and Care Research (NIHR) is funded by the Department of Health and Social Care (DHSC) to transform research in the health and social care system, including through support for NHS research. Research led to the first proven treatments for Covid, for example the use of dexamethasone, estimated to have saved over a million lives worldwide . This success was in part due to how research is undertaken in the unique environment of the NHS, innovative trial designs, the support provided by the NIHR, frontline staff enabling research, and the awareness and readiness of the public to support research. We need to learn from these and other successes, and translate this across all health and care settings. ICSs will play a vital role in enabling research to be embedded in evolving patient pathways across their footprints.
Example: PRINCIPLE trial – finding treatments for Covid recovery at home
The Platform Randomised Trial of Treatment in the Community for Epidemic and Pandemic Illnesses (PRINCIPLE) was a UK-wide, clinical study to find Covid treatments for recovery at home without the need to attend hospital. The study was open to all with ongoing Covid symptoms, registration was easy, and the trial was run entirely remotely by delivering ‘participant packs’ to people’s homes. It was one of the first trials in the world to show that azithromycin and doxycycline did not benefit patients with Covid and to identify the effectiveness of a commonly used drug – inhaled budesonide –in reducing time to recovery.
The PRINCIPLE study team demonstrated the integral role that primary, secondary and ambulatory care staff can play in the delivery of studies. Local collaborators were trained in good clinical practice to allow them to assess and confirm the eligibility of potential participants, and were commended specifically for their use of patient data to contact people soon after they received a positive test result. It is this network of local staff contributing to research within their healthcare setting that has enabled over 10,000 people to be recruited onto this study so far – one of the largest at home Covid treatment studies worldwide.
This is an example of a study design that incorporates the vital contributions of healthcare providers across the system.
Policy-makers and commissioners need evidence to support their decision-making around the delivery and system-wide transformation of health and care services, including how health inequalities will be reduced.
There is also evidence that:
- staff involved in research have greater job satisfaction and staff turnover is lower in research active trusts ( Academic factors in medical recruitment: evidence to support improvements in medical recruitment and retention by improving the academic content in medical posts)
- research active hospitals have lower mortality rates, and not just among research participants ( Research activity and the association with mortality )
- 83% of people believe that health research is very important ( Survey of the general public: attitudes towards health research)
- healthcare performance improvements have been seen from the creation of academic research placements ( Experiences of hospital allied health professionals in collaborative student research projects: a qualitative study )
- clinical academic research, and in particular the practice changes resulting from it, is associated with improved patient and carer experiences ( A qualitative systematic review and thematic synthesis exploring the impacts of clinical academic activity by healthcare professionals outside medicine ).
Key to having research embedded in health and care is having staff who can understand, undertake, use and generate new research, and share actionable research finding as part of a pro-research culture. Education and training are therefore critical for research to be sustainably embedded within health and care, and for people to develop careers in research and support it in their clinical or care roles.
DHSC, NHS England, the devolved administrations, NIHR and other partners expect to publish a clinical research workforce strategy in 2023/24 to help the UK realise the national clinical research vision outlined in Saving and Improving Lives: The Future of UK Clinical Research Delivery and deliver the Life Sciences Vision to see research embedded in the NHS as part of health and care pathways.
Research will support ICSs to deliver on their four key aims:
Improving outcomes
The NHS 2023/34 priorities and operational planning guidance emphasises the importance of research in improving patient care, outcomes and experience.
Research evidence will inform commissioning decisions to improve experience and outcomes. Research activities should align with the local health priorities identified through local joint strategic needs assessments, and may be best designed and delivered by collaborating with partners. Research priorities may be best addressed by collaborating with partners nationally to design and deliver research.
Tackling inequalities
Research can give a better understanding of local populations and the wider determinants of health, and with this the steps to maintain health and narrow health inequalities.
Enhancing productivity
The development of ICSs creates the opportunity to consider research delivery within the ICS and across ICS boundaries, increasing flexibility of workforce or recruitment while reducing bureaucracy and improving research productivity and value for money.
Supporting social and economic development
An active research ecosystem working in a co-ordinated way and to national standards brings revenue and jobs to regions. The NIHR Clinical Research Network (CRN) supports service users, the public and health and care organisations across England to participate in high-quality research. The 2019 impact and value report detailed the significant income and cost savings that commercial research generates for NHS trusts. Between 2016/17 and 2018/19 the NHS received on average £9,000 per patient recruited to a commercial clinical trial and saved over £5,800 in drug costs for each of these patients. This equates to income of £355 million and cost savings of £26.8 million in 2018/19.
In 2021 150 members of the Association of Medical Research Charities funded £1.55 billion of medical research, including the salaries of 20,000 researchers. Every £1 million spent by charities on medical research in the UK contributes £1.83 million to the economy.
Example: Research that cut problematic prescribing and generated cost savings in general practice – a local health priority
Analysis of routine patient data identified the need for strategies targeting clinicians and patients to curb rising opioid prescribing. From this, the Campaign to Reduce Opioid Prescription (CROP) was launched in 2016, urging GPs across West Yorkshire to ‘think-twice’ before prescribing opioids. This promoted the NICE guidance on chronic pain , which recommends reducing the use of opioids because there is little or no evidence that they make any difference to people’s quality of life, pain or psychological distress, but they can cause harm, including possible addiction.
Over a year 15,000 fewer people were prescribed opioids (a 5.63% relative reduction), a net saving to the NHS of £700,000. The biggest reduction was in people aged over 75, who are at higher risk of opioid-related falls and death, and there was no compensatory rise in the prescribing of other painkillers or referrals to musculoskeletal services.
The CROP campaign, led by researchers at the University of Leeds, has subsequently been rolled out across all ICBs in Yorkshire and the Humber, and the North East and North Cumbria ICB, and the 1,045 practices to which it has been delivered are reporting results similar to the above.
Foy R, Leaman B, McCrorie C, Petty D, House A, Bennett M, et al (2016) Prescribed opioids in primary care: cross-sectional and longitudinal analyses of influence of patient and practice characteristics | BMJ Open 69(5).
Alderson SL, Faragher TM, Willis TA, Carder P, Johnson S, Foy R (2021) The effects of an evidence- and theory-informed feedback intervention on opioid prescribing for non-cancer pain in primary care: A controlled interrupted time series analysis. PLOS Med .
2. ICS, ICP and ICB responsibilities and requirements
ICBs have legal duties and other requirements that relate to research. These are additional to the duties and responsibilities of individual providers within ICS footprints. This section sets out what these duties mean in practical terms and gives examples of how to meet them.
2.1 Legal duties relating to research in the Health and Care Act 2022
Part 1 of the 2022 Act includes specific legal duties for ICBs and NHS England in respect of research. In the Explanatory Notes to the 2022 Act, government sets out how ICBs could discharge their research duty.
Duty to facilitate or otherwise promote research
The ICB duty builds on the previous clinical commissioning group (CCG) duty to promote research, by requiring each ICB, in the exercise of its functions, to facilitate or otherwise promote research on matters relevant to the health service. This duty is intended to include a range of activities to enable research. Section 3 of this guidance outlines ways in which ICBs can do this.
The NHS Constitution also makes clear that patients should be enabled to take part in research: “the NHS pledges … to inform you of research studies in which you may be eligible to participate”.
The Provider Selection Regime (PSR) will be a new set of rules for arranging healthcare services in England, introduced by regulations made under the 2022 Act. The research component should be referred to once the PSR is published.
Duty to facilitate or otherwise promote the use in the health service of evidence obtained from research
This duty similarly builds on the CCG requirement to promote the use of evidence. ICBs must, in the exercise of their functions, facilitate or otherwise promote the use in the health service of evidence obtained from research. For example, ICBs should facilitate or otherwise promote the use of evidence in care, clinical and commissioning decisions.
Duty for ICSs to include research in their joint forward plans and annual reports
Joint forward plans are five-year plans developed by ICBs and their partner NHS trusts and foundation trusts. Systems are encouraged to use the joint forward plan as a shared delivery plan for the integrated care strategy and joint health and wellbeing strategy, aligned to the NHS’s universal commitments. The plan must explain how the ICB will discharge its duties around research, and the ICB must report on the discharge of its research duties in its annual report. These inclusions will raise the profile of research at board level and help embed research as a business-as-usual activity.
The joint forward plan and NHS Oversight Framework guidance set the minimum requirements for what needs to be included in plans and reports.
NHS England duty to include how each ICB is carrying out its duties relating to research in its annual performance assessment of each ICB
NHS England has a new legal duty to annually assess the performance of each ICB and publish a summary of its findings. For 2022/23 NHS England will complete a narrative assessment, identifying areas of good and/or outstanding performance, areas for improvement and any areas that are particularly challenged, drawing on national expertise as required and having regard to relevant guidance. This assessment will include a section considering how effectively the ICB has discharged its duties to facilitate or otherwise promote research and the use of evidence obtained from research.
This, alongside the implementation of the NHS Long Term Plan commitment to develop research metrics for NHS providers, will increase transparency across the system and enable more targeted support for research. Research metrics from NHS England, the Care Quality Commission (CQC) and NIHR will enable the monitoring of progress over time, and are under development with sector colleagues, including providers.
2.2 Legal requirement to work with people and communities
Working with people and communities is a requirement of ICBs, and statutory guidance is available to support them and their partner providers meet this legal duty. A co-ordinated approach across healthcare delivery and research will make it more likely that research reflects what matters to people and communities.
This will also help ICBs to fulfil their legal duty in the 2022 Act to reduce health inequalities in access to health services and the outcomes achieved. Section 3.9 includes links to resources to help guide engagement with underserved communities around research.
The Public Sector Equality Duty also applies and requires equality of opportunities between persons who share a relevant protected characteristic and persons who do not.
2.3 Research governance
While research can address local priorities, it typically operates across ICS boundaries and at national and international levels. Health and social care research is governed by a range of laws, policies, and international, national and professional standards.
The Health Research Authority (HRA ) is responsible for ensuring such regulation is co-ordinated and standardised across the UK to make it easier to do research that people can trust. The HRA is an executive non-departmental public body created by the Care Act 2014 to protect and promote the interests of patients and the public in health and social care research, including by co-ordinating and standardising the practice of research regulation. Local authorities and the NHS are obliged to have regard to its guidance on the management and conduct of research.
Before a research project can start in the NHS in England it must receive approval from the HRA. This includes research taking place in NHS trusts, NHS foundation trusts, ICBs or primary care providers of NHS commissioned services in England, and all research under an NHS duty of care, including that undertaken by NHS staff working in social care or other non-NHS environments.
The HRA schemes indemnify NHS organisations accepting these assurances against any claim covered by the NHS Litigation Authority arising as a result of incorrect assurances. If an NHS organisation duplicates the HRA assessments, it will be liable for any consequences of the decisions it bases on its own checks.
ICBs and partner organisations should have processes for the set up and delivery of research that comply with national laws and systems, and does not duplicate them. Such national systems include confirmation of capacity, National Contract Value Review (NCVR), management of Excess Treatment Costs (ETCs) and contracting arrangements (see section 2.4).
The UK Policy Framework for Health and Social Care sets out the roles and responsibilities of individuals and organisations involved in research.
2.4 Contractual requirements around research
NHS England mandates commissioner use of the NHS Standard Contract for all contracts for healthcare services other than primary care. The contract is updated annually. References to research in the current NHS Standard Contract and service conditions fall into three main areas.
Recruitment of service users and staff into approved research studies
The NHS Standard Contract obliges every provider of NHS-funded services to assist the recruitment of suitable subjects (whether patients or staff) into approved research studies. This requirement aligns to those in the 2022 Act that require ICBs to facilitate or otherwise promote research (see section 2.1). Section 3 considers how this requirement can best be met. Research involving people or their data requires ethical and potentially other approvals (see section 2.3).
National Directive on Commercial Contract Research Studies
Adherence to the National Directive is mandated as part of the NHS Standard Contract. The directive states that providers must:
- Use the unmodified model agreements for sponsor-to-site contracting; HRA and Health and Care Research Wales (HCRW) approval of studies will be dependent on use of these templates.
- Use the standard costing methodology to set prices for commercial contract research undertaken by NHS providers; this is currently in the NIHR interactive costing tool (NIHR iCT).
- Introduce the National Contract Value Review (NCVR) process in line with national rollout. NCVR is a standardised national approach to costing commercial contract research within the NHS. It currently covers acute, specialist and mental health trusts, but the intention is to roll it out to all NHS providers. The creation of ICSs is the ideal opportunity to explore how commercial study set up can be supported across these footprints, reducing the resource needed and time taken.
Comply with HRA/NIHR research reporting guidance
The provider must comply with HRA/NIHR research reporting guidance, as applicable.
2.5 Excess treatment costs
Patients in a research study may receive healthcare that differs from what is standard in the NHS, requires more clinician time or is delivered in a different location. The associated NHS treatment costs may exceed or be less than those of standard treatment. If greater, the difference is referred to as the NHS Excess Treatment Costs (ETCs).
In the case of commercial contract research, the commercial funder will pay the full cost of the study. In the case of non-commercial research, the commissioner of the service in which the study operates is responsible for funding the ETCs.
ICBs as commissioners of services are responsible for ETCs in services that they commission. Guidance for the management of ETCs is available.
DHSC and NIHR are piloting interim arrangements to support non-NHS ETCs for research in public health and social care (non-NHS intervention costs). Please refer to the further detail on the NIHR website .
2.6 Care Quality Commission
The CQC is currently developing its approach for ICS-level assessments, and its new assessment framework will be introduced towards the end of 2023 .
CQC inspection of NHS providers continue, with research assessed as part of the review of the trust-level Well-led framework. Providers are asked:
- Are divisional staff aware of research undertaken in and through the trust, how it contributes to improvement and the service level needed across departments to support it?
- How do senior leaders support internal investigators initiating and managing clinical studies?
- Does the vision and strategy incorporate plans for supporting clinical research activity as a key contributor to best patient care?
- Does the trust have clear internal reporting systems for its research range, volume, activity, safety and performance?
- How are service users and carers given the opportunity to participate in or become actively involved in clinical research studies in the trust?
3. Developing a research strategy
3.1 why develop a research strategy.
Like the health and care system, the research environment is complex. Developing a research strategy will help bring together the legal and other duties around research in a coherent way, and help the ICS understand its local research capability, workforce, activity and needs, set ambitions around research and maximise the benefits associated with commercial research. It will help demonstrate the benefit of research locally, nationally and internationally, and guide the production of clear plans.
Example: Value of research partnerships and integration with ICSs
Bristol Health Partners (BHP) Academic Health Science Centre (AHSC) has a fully integrated relationship as the new Research and Innovation Steering Group for the Bristol, North Somerset and South Gloucestershire (BNSSG) ICS, and reports directly to ICB chief executives.
The group provides the strategic direction and oversight for all research undertaken and delivered across the system. Membership includes directors of research, clinical strategy, public health, social care, senior innovation and education leaders from its core funding partners. It also includes public contributors and senior representatives from primary care, NIHR Applied Research Collaboration West, NIHR CRN West of England, West of England Academic Health Science Network (WEAHSN), Healthier Together ICS, university research institutes and People in Health West of England.
The group has reviewed ICS programmes, identified current and potential research and innovation connections, and begun to establish new connections. It has also supported work with the ICS Ageing Well programme and secured funding for innovative pilots to improve dementia care and increase physical activity for older adults.
Since 2016 BHP has directly contributed an estimated additional £1.1 million to support ICS priorities through Health Integration Team projects and other activities, and has attracted more than £33 million of external research, service redesign and infrastructure into the region.
3.2 General considerations
In developing its research strategy, the ICS may find it helpful to consider these overarching questions alongside the suggested focused content covered in the sections below:
- What do you hope to achieve within a given timeframe?
- Are all the right organisations involved in developing the research strategy?
- How will the health and care workforce be enabled to deliver the research strategy?
- How can research be embedded in existing health and care delivery and pathways?
- What mechanisms are in place to translate actionable research findings into practice and decision-making?
- What inequalities exist in different areas, communities or groups? How will you ensure planning and delivery of research aligns to CORE20plus5 priorities?
- Are you considering equality, diversity and inclusivity and the Public Sector Equality Duty in facilitating and promoting research opportunities for service users and for health and care staff?
- Is the ICS considering the opportunities of developing their commercial research portfolio?
- Is research informing or being informed by population health management?
- How will you plan and deliver research in a sustainable manner, aligning it to the Greener NHS agenda and the ICB’s duties in relation to climate change ?
Buy-in from NHS staff, patients and the public will be vital if ICBs are to discharge their research duties and deliver on their research plans. An important consideration is how to develop sustainable, routine and accessible information flows to ensure the ICB, partners, staff, patients and public can access up-to-date and appropriate information around local research activity, regional, national and international research opportunities and findings, and contact information.
3.3 Leadership and governance across the ICS
Executive leadership.
The Explanatory Notes to the 2022 Act suggest that ICBs have board-level discussions on research activity, the use of the evidence from research, the research workforce and research culture within the ICS. ICSs should refer to the NHS Leadership Competency Framework for board-level leaders at organisation and ICS level for the competencies relating to the research duties of ICSs, once published.
All ICBs are encouraged to have an executive lead responsible for fulfilling the research duties conferred by the 2022 Act. They should help give the ICB a clear understanding of research across the area, regularly reporting on progress towards agreed aims. An executive lead can take responsibility for ensuring clear research ambitions and a research strategy are developed; oversight of organisational research portfolios, diversity in research, alignment to national priorities; promotion of research skills and the need for research skills training; and succession planning.
Senior leaders could engage, consult and be supported by representatives of each registered health and social care professional group when developing strategic plans, and for oversight of training, succession planning, and equality and inclusivity. They could use the capacity and capability of the research and development leads within provider organisations, although established lead roles across social care settings are rare so extra effort may be needed to garner social care research insight.
Research steering group, board or forum
Some CCGs had research steering groups and some of these have expanded with the widening remit of ICBs. ICSs that do not have a such a group should consider adopting a model similar to one in other ICSs where research is effectively embedded in ICS governance structures.
A dedicated steering research group, board and/or forum can:
- provide dedicated time to plan, oversee and report on research
- bring a range of representatives from research infrastructure organisations, patients and the public together with representation from across the ICS, to develop a common aim and objective
- ensure board-level sight of research
- take a cross-ICS approach to research, increasing participation and diversity in research, and reducing bureaucracy.
Example: A dedicated research and innovation subgroup
East and North Hertfordshire Health Care Partnership established a formal research and innovation subgroup to support its objectives to transform services, reduce health inequalities and improve patient health and wellbeing. This subgroup is dedicated to determining and supporting local research priorities and developing an innovation agenda. With effective patient and public involvement, it is working to ensure the local population has access to more research opportunities.
Bringing together the NIHR, academia, industry and local health and care services, the subgroup develops collaborative work plans that support the design, implementation and evaluation of local transformation needs, sharing resources, staff, expertise and facilities. Its work exemplifies a sustainable approach to partnership working and supports Hertfordshire and West Essex ICS’s developing strategy.
HWE ICS Partnership Board 14 September 2021
3.4 Understanding your research activity and working with local and national research infrastructure
Research in NHS and non-NHS settings across an ICS footprint will be supported by different organisations. In some areas networks or collaboratives already exist to bring these organisations together, but in others the links are not as well formed. ICBs would benefit from having a clear map of the research infrastructure and pre-existing local or national investment into research in their area.
It may be valuable to consider:
- Who are the research leaders in your local health and care system, NIHR, higher education institutions, VCSE sector and businesses?
- Are there any pre-existing local or regional research, researcher or research engagement networks?
- What are the opportunities to inform, participate in, collaborate with or lead national and international research efforts in addition to local opportunities?
A list of organisations involved in research including NIHR-funded infrastructure and programmes is included in Annex 1 .
Much of the research undertaken in NHS and other health and care settings is funded though national calls and grants provided by funders such as NIHR, research charities , UK Research and Innovation (UKRI) , including the Medical Research Council (MRC ) and Economic and Social Research Council (ESRC) , and is aligned to national priorities. Other research may include national or international commercial or non-commercial clinical trials funders.
Partners within ICS systems can use NIHR research portfolio data to monitor and plan research activity; however, not all research is included within the NIHR’s portfolio, so this will not give a full picture of the research within the footprint. Mechanisms to map and monitor research more widely could be incorporated in ICB research strategies.
Some local needs may best be addressed through public health or social care research rather than research in primary, secondary or tertiary healthcare settings. Public health and social care research are described in Annex 2 .
Example: Mapping health and care research activity, expertise, interests and infrastructure
The Nottingham and Nottinghamshire Integrated Care System Research Partners Group meets bi-monthly and is chaired by the ICB Head of Research and Evidence. It brings together senior managers from the NHS providers, ICB, two local authorities, two universities and the NIHR CRN East Midlands, providing a forum for ICS-wide research discussions and the development of a system-wide collaborative approach to health and care research across the ICS. Among its aims, the group seeks to increase participation in research at both the organisational and population level, enable equity of access to research opportunities and generate impact on health and care pathways.
The group have mapped health and care research activity, expertise, interests and infrastructure in the constituent organisations. With this the ICS can see the research capabilities, strengths, expertise, and areas of synergy and opportunities for future collaboration that align to its needs and priorities, and also gaps for future development, recognising that organisations are at different stages of research development.
3.5 Understanding local needs
Universal NHS priorities will be reflected in local research needs, and each ICS footprint is likely to have its own specific local research needs. Joint strategic needs assessments (JSNAs) are undertaken jointly by local authorities and ICBs through health and wellbeing boards (HWBs) to identify current health and social care needs of local communities, where more information is needed to do so or to understand how best to address the need. People and communities should be directly involved in identifying local need, including by working with local charities, specific communities or groups who face inequalities in access to, experience of or outcomes from healthcare, eg to target health research at those areas and populations with greatest need.
ICPs are required to develop an integrated care strategy informed by JSNAs and the joint health and wellbeing strategy (JHWS). The integrated care strategy sets out how the assessed needs can be met through the exercise of the functions of the ICB, partner local authorities or NHS England, and is informed by research and practice-based evidence, as stated in the health and wellbeing guidance. In considering where such evidence is lacking, HWBs should identify in JSNAs those research needs that ICBs, local authorities and NHS England could meet through the exercise of their research functions.
Systems are encouraged to use their joint forward plan to develop a shared delivery plan for the Integrated Care Strategy and the JHWS that is supported by the whole system, including local authorities and VCSE partners. ICBs and trusts must also use their Joint Forward Plan to describe how the ICB will discharge its duty in respect of research.
The Explanatory Notes to the 2022 Act suggest how ICBs can discharge their duties around research. These include the articulating local research needs when assessing local needs and how they will be addressed when preparing strategies and plans, and encouraging partner organisations to play an active and collaborative role in pursuing these.
3.6 Supporting delivery of research
Once an ICS has a clear picture of its local research infrastructure it can consider how best to target and support research and the research workforce across its footprint and how research findings will be used. For this, the ICB should ensure that its approaches reflect national approaches to costing, contracting, approvals and information governance, and that they are also informed by learning from effective practices across equivalent ICBs.
As healthcare shifts into communities, ICSs should support the parallel shift in research by embedding research in health and care. Increasing access to research opportunities will give service users earlier access to new treatments, and faster research set up and delivery may provide the evidence needed to support improvements to local care sooner. Inclusive recruitment practices will be needed to ensure that all groups in society have the opportunity to help shape and take part in research, and benefit from research findings.
In developing its research strategy, an ICS has opportunities to reduce bureaucracy, and make research more efficient and effective across its own and with other ICS footprints, and across NHS and non-NHS boundaries, while meeting national regulatory guidance. ICBs will be expected to work with the HRA to co-develop, build on and implement strategies for further co-ordination and standardisation of study set-up and delivery processes. Any regional systems and processes that ICBs do establish must support consistent national practice in relation to the management and regulation of research, and should not duplicate them. The HRA will work with ICBs to address barriers to efficient and rapid study set-up, including model agreements, information governance and R&D office functions.
Other potential areas for streamlining and cross-organisational working include:
- cross-ICS research proposals to identify research needs
- research delivery – identifying how ICS-wide approaches could accelerate patient recruitment and deployment of research delivery staff
- shared data architecture, including the NHS Secure Data Environment for Research Network and its subnational secure data environments (SDEs). Subnational SDEs cover multiple ICSs to achieve access to multimodal data at a scale of approximately 5 million citizens, and over time will achieve technical and governance interoperability
- a greater focus on translation and implementation of research findings into health and care practice, supporting faster improvements
- sharing access to and funding for knowledge and library services
- shared processes and repositories for research assets.
The Explanatory Notes to the 2022 Act suggest that one way an ICB could discharge its research duty would be to have a dedicated research office or team supporting research.
3.7 Enabling cross-provider research
Health and care priorities can often only be addressed with complex, multiorganisational approaches and as such the research to inform these needs to span organisational boundaries. Organisational policies should promote cross-organisational research and dissemination of research findings, including through participation in collaborative research to address national priorities, joint staff posts, honorary contracts, and administratively easier movement of researchers between health and care organisations and other sector partners, including higher education, industry, charities and local authorities.
The HRA and ICS partners are developing national guidance to support cross-provider research.
The NIHR CRN can offer ICSs opportunities to participate in national and international research studies, including those the NIHR, industry and others commission.
3.8 Commercial research
Commercial contract research is research funded solely by industry, where NHS providers are contracted to carry out the research. Most of these research studies in the NHS are interventional clinical trials, such as the NHS-Galleri trial and Astra Zeneca’s COVID-19 vaccine development . Commercial research can give patients access to a wider range of research opportunities, earlier access to novel therapies and treatments, provide drugs free of charge to patients in trials, accelerate the development of new treatments and devices, generate income for providers, and fund NHS staff. It is vitally important for the benefit of patients, the NHS and the UK economy that we create an environment in the NHS that makes it easy and efficient for the NHS to undertake commercial research. This is particularly important when it comes to international commercial research, where companies can place their studies in a number of different countries and consideration of anticipated set up and recruitment times informs where they place trials.
Data gathered during some commercial research is specific to the study and is the property of the company, as is any Intellectual Property (IP) generated. In other cases, where the NHS contributes to the foreground IP – such as through the use of NHS data for research or where NHS expertise provides important contributions to a commercial product – it is important that the NHS shares in the value of IP generated as a consequence of its contributions.
The establishment of ICSs is an ideal opportunity for their creation of ambitions to enable, grow and benefit from commercial research. ICSs should explore how efficient commercial study set up and delivery could be streamlined across sites within their footprint, and should set ambitions around commercial research.
3.9 Involving patients, service users, carers and the public in research
In developing a research strategy ICSs should set out their approach to diverse public and patient involvement (PPI) in relation to research.
Areas where working with people and communities could add value in the context of research include:
- identification of local research needs, including through JSNAs and JHWSs
- designing research proposals in partnership with local or national experts
- raising awareness of research opportunities and recruitment of participants
- developing research outcome reports and identification of how and when participants will be able to access these
- consideration of how members of the public can access the outputs from publicly-funded research
- how volunteers should be involved and what they should be paid.
The UK Standards for Public Involvement sets out the core components of good public involvement. A guide outlining good practice in engaging underserved communities around research is available from NHS England. Resources about good practice around PPI in designing and delivering research, including around incentivisation , are also available from the HRA and NIHR .
It will be useful to link into established community involvement approaches. NIHR infrastructure organisations may have established networks of expert PPI representatives, and ICSs have extensive VCSE Alliances. A co-ordinated community engagement approach across health and care delivery and research will reduce the risk of overburdening communities with organisations wanting to work with them, and will support the identification of under-served communities.
3.10 Ensuring anyone can participate in research
Making research more visible within communities and increasing the public’s understanding of research can ensure greater diversity in research participation. Research findings will then be more generalisable to a broader range of groups or communities, or can be targeted and specific to relevant communities.
ICSs should seek mechanisms to ensure that opportunities to take part in research are available to all. They should consider encouraging patients and members of the public to register on NIHR Be Part of Research (a national registry where people can express their interest in being contacted about research that is relevant to them), widely disseminate research opportunities and make provision for inclusive access for communities to take part in research. Decentralised or virtual trials are remote access trials recruited to and delivered using electronic tools, making it easier for people to participate in some studies without needing to visit a recruiting hospital or attend appointments in person. ICBs should consider ways in which research delivery can increase access to research opportunities for people within their area. ICBs should also advise the public how they can access research outputs.
NIHR and UK Research and Innovation provide resources that help organisations address issues of equality, diversity and inclusion in research settings.
Example: RELIEVE-IBS decentralised trial
In 2020, Newcastle researchers launched RELIEVE-IBS, one of the first interventional decentralised clinical studies in the UK to trial Enterosgel, a new treatment for irritable bowel syndrome with diarrhoea (IBS-D). Decentralised trials are remote access trials that use electronic tools for trial recruitment and delivery, without the patient needing to visit a recruiting hospital site, which could be miles from their homes – a convenient option for patients with IBS-D. By running the trial remotely, researchers could reach beyond the small proportion of those with this condition who attend specialist clinics, as well as save resource for the sponsor.
Not only did this trial embrace technological developments to deliver research, but it empowered more patients to become involved regardless of where they lived. With in-depth patient input, the research team were able to shape the recruitment approach to be highly accessible to participants and were offered feedback on how to refine the trial design by the sponsors. The resulting patient-centric design ensured a good recruitment response when the trial opened.
NIHR (2020) Virtual trial recruits 67% faster led by NIHR Patient Recruitment Centre in Newcastle in collaboration with Enteromed
NIHR (2021) Pushing virtual boundaries to improve patient engagement and accessibility
NIHR (2022) RELIEVE IBS-D trial case study
3.11 Health data in research
Health data generated through care of service users in the NHS can fuel a revolution in the research and development of new diagnostics and treatments, maximising the potential to improve service user outcomes and experiences, support diversity in research, and minimise health inequalities through research. To do this, researchers need access to high quality and timely data to generate insights. The public expect data to be used legally and efficiently to conduct and support research.
National commitments around data for research can be found in Data saves lives: reshaping health and social care with data . This strategy shows how data will be used to bring benefits to all parts of health and social care. To achieve this vision, the NHS will be making a strategic move away from a system of data dissemination to one of data access when making NHS health and social care data available for research and analysis. This will be facilitated by the implementation of secure data environments (SDEs).
SDEs are data storage and access platforms with features that enable organisations to have greater control and oversight over their data. SDEs allow approved users to view and analyse data without it having to leave the environment. The SDE policy guidelines provide a clear signal to the sector that SDEs will become the default way of accessing NHS data for research.
This change is supported by major investments in digital infrastructure through the Data for Research & Development Programme, which is funding the development of national and subnational SDEs. The subnational SDEs will cover the entirety of England and individual platforms will cover several ICS.
ICBs should seek ways to promote and enable the use of these rich data sources for research and include them in their research strategy.
3.12 Using evidence for planning, commissioning and improving health and care
Evidence-based commissioning has advantages for the commissioner, workforce and service users, as it can:
- lead to innovation in service design and delivery
- enhance the quality of health and care provision
- reduce clinical variation between locations and providers
- improve equity of access to services
- improve patient and population outcomes.
As part of the commissioning process, commissioners are expected to use evidence-based clinical policies, as per the Roadmap for integrating specialised services within integrated care systems . Knowledge and library services can help source and interpret evidence.
The Provider Selection Regime will reflect the research duties of the 2022 Act and should be referred to when commissioning provider services, once it has been published.
NHS knowledge and library services provide access to evidence and support for knowledge management; they train people in searching for, handling and publishing information. The Knowledge for Healthcare strategy encourages and equips NHS knowledge and library services to support NHS organisations with the translation of knowledge for the spread and adoption of research and innovation. To fulfil their obligations under the 2022 Act, ICBs could commit to active knowledge translation.
Evidence for commissioning information is available from a number of sources:
- NHS Library and Knowledge Hub
- Health Libraries and Information Services Directory
- NICE guidance
- NIHR evidence
- NHS evidence works toolkit
- Academy of Medical Royal Colleges: Evidence-based Intervention
- A million decisions
The infographic for the role of research and evidence in commissioning also provides sources for evidence-based commissioning.
Example: Evidence mobilisation, knowledge sharing and improving outcomes
The STEMClub (Sustaining Transformation by Evidence Mobilisation) is a network in the North East and North Cumbria that brings together local policy and decision-makers with NHS knowledge and library specialists to facilitate evidence-based decision-making. The input of knowledge specialists ensures timely access to published research and provides knowledge management expertise to shape how soft intelligence is translated into knowledge assets.
As members within the STEMClub network, knowledge and library specialists are providing ongoing detailed evidence reviews and information management expertise to facilitate system-wide working , eg:
- North East North Cumbria Frailty Framework
- North East and North Cumbria Maternity Clinical Network
- a review of optimal patient transfer times in the North East and North Cumbria
- regular evidence summaries for the ICS Mental Health Evidence and Evaluation subgroup.
3.13 The health and care workforce and research
Staff involved in research have greater job satisfaction and research active trusts have lower staff turnover [3] . Clinical academic roles [7] , having research colleagues within services [8] and taking students on research placements [6] are felt to foster an increase in knowledge and skills across the wider staff workforce. The General Medical Council (GMC) and the Royal College of Physicians (RCP) and NIHR have issued position statements and recommendations around research, with additional signatories including UKRI, UKRD, the Academy of Medical Royal Colleges and the Royal College of Surgeons of England. Learning resources, including programmes for ongoing professional development of the research delivery workforce, are available through NIHR Learn.
In developing a research strategy ICSs could ensure that, as part of their people function and approach to workforce planning :
- Staff roles in leading, delivering or facilitating research and in supervising those developing research skills are recognised, supported and enabled across all staff groups and health and care settings as part of a positive research culture.
- The value of evidence is recognised, and education and training around research are facilitated. Opportunities to develop research careers or in overseeing the development of other researchers are enabled; this may include having protected time, inclusion in job plans and joint appointments across health and care providers and academic institutions.
- Ensuring that there is capacity and systems that support research through services like imaging, pathology and pharmacy, as well as finance and human resources.
- Individual organisations do not always have the necessary skills or services to support effective research and its impact, such as IP management, methodological expertise, regulatory compliance, statistical analysis, knowledge mobilisation expertise, genomics expertise, health informatics and data analytics. Mechanisms are needed to ensure that these can readily and rapidly be accessed across other health and care organisations, including from local authorities and other non-NHS care providers.
A UK Clinical Research Workforce Strategy is under development. ICSs should update their approaches to their research workforce once DHSC publishes this in 2023/24.
Example: Investing in the research workforce – developing capacity for chief investigators
Across the West Midlands NIHR CRN, an investment of approximately £750,000 to develop capacity for chief investigators returned additional research grant income of over £18 million in three years. This was achieved primarily by increasing the programme activity for consultants in areas where chief investigators were underrepresented.
The funding was provided through a competitive process and co-supported by the local NIHR CRN, with several local trusts jointly funded these scholars.
Kirk J, Willcocks J, Boyle P, Brocklehurst P, Morris K, Kearney R, et al (2022) Developing chief investigators within the NHS: the West Midlands clinical trials scholars programme. Clin Med 22(2): 149–52.
Kirk J, Reynolds F, Adey E, Boazman M, Brookes M, Brocklehurst P (2022) Developing paediatric chief investigators within the NHS: the Clinical Trials Scholars programme . Arch Dis Child Educ Pract Published online first: 22 February 2022. doi: 10.1136/archdischild-2021-322186
4. References
- Varnai P, Rentel M, Dave A, De Scalzi M, Timmerman W, Rosemberg-Mantes C, Simmonds P, Technopolis Group (2017) The impact of collaboration: The value of UK medical research to EU science and health .
- Boaz A, Hanney S, Jones T, Soper B (2015) Does the engagement of clinicians and organisations in research improve healthcare performance: a three-stage review. BMJ Open 5: e009415. doi:10.1136/ bmjopen-2015-009415 .
- Rees MR, Bracewell M (2019) Academic factors in medical recruitment: evidence to support improvements in medical recruitment and retention by improving the academic content in medical posts. Postgrad Med J 95(1124): 323-327. doi:10.1136/postgradmedj-2019-136501 .
- Ozdemir BA, Karthikesalingham A, Singha S, Poloniecki JD, Hinchliffe RJ, Thompson MM, et al (2015) Research activity and the association with mortality. PLoS ONE 10(2): doi.org/10.1371/journal.pone.0118253 .
- Hunn A (2017) Survey of the general public: attitudes towards health research . Health Research Authority.
- Angus RL, Hattingh HL, Weir KA (2022) Experiences of hospital allied health professionals in collaborative student research projects: a qualitative study. BMC Health Services Research 22(1). Available at: https://doi.org/10.1186/s12913-022-08119-7 .
- Newington L, Wells M, Adonis A, Bolten L, Bolton Saghdaoui L, Coffey M, et al (2021) A qualitative systematic review and thematic synthesis exploring the impacts of clinical academic activity by healthcare professionals outside medicine. BMC Health Serv Res 21(1). Available at: https://doi.org/10.1186/s12913-021-06354-y .
- Wenke RJ, Hickman I, Hulcombe J, Phillips R, Mickan S (2017) Allied health research positions: A qualitative evaluation of their impact. Health Res Policy Syst 15(6). Available at: https://doi.org/10.1186/s12961-016-0166-4
Annex 1 – Organisations that may be involved in regional or local research
- Clinical Research Networks (CRNs) , which will be retendered and renamed regional research delivery networks (RRDNs) from April 2024
- Applied Research Collaborations (ARCs)
- Biomedical Research Centres (BRCs)
- Experimental Cancer Medicine Centres (ECMCs) , jointly funded with Cancer Research UK
- Research Design Services (RDSs) and Clinical Trials Units (CTUs) which will be replaced by the NIHR Research Support Service from 1 October 2023
- Patient Recruitment Centres (PRCs)
- MedTech and In vitro diagnostic Co-operatives (MICs) , which will be replaced with HealthTech research centres from April 2024
- School of Public Health Research, School of Primary Care Research and School of Social Care Research
- Health Determinants Research Collaborations (HDRCs)
- Clinical Research Facilities (CRFs)
- Patient Safety Research Collaborations (PSRCs)
- Translational Research Collaborations (TRCs)
- Academic Health Science Centres (AHSCs)
- university teaching hospitals and all trusts that deliver research activity
- primary care organisations, including GP practices, that deliver research activity
- higher education institutions (HEIs)
- local authorities
- social care partners
- Local Government Association
- local and national charities that fund, collaborate in or support participation in research
- research and development offices in providers or CSUs, including primary care providers and ambulance, community and mental health trusts, and those in the VCSE sector
- UKRD members
- NHS subnational secure data environments for research
- NHS R&D Forum
- NHS Genomic Medicines Service Research Collaborative
- NHS Knowledge and Library Services
- Academic Health Science Networks (AHSNs) are often well linked with research organisations and infrastructure as part of their roles in development, adoption and spread of innovation.
Annex 2 – Public health and social care research
Public health research investigates issues that impact at a population rather than an individual level. This can be done within the NHS with system-level studies, such as secondary prevention of cardiovascular disease and examining the impact on health inequalities of changes to the NHS resource allocation formula, and outside the NHS for the wider determinants of health such as air quality, transport systems and housing. There is a substantial body of public health evidence for the clinical and cost effectiveness of prevention, health protection, health service redesign and addressing health inequalities.
Social care research aims to improve the lives of children and adults who need to draw on personal or practical care and support, and family members or other unpaid carers. It can include research around the introduction, use and impact of technologies, and changing social care interventions, policies and practice. Social care research also examines issues pertaining to the safeguarding of adults and children and workforce, commissioning of services, and questions about organisational and professional practice, including decision-making, training and the quality of care.
Publication reference: PR1662
- Search Menu
- Sign in through your institution
- Advance Articles
- Editor's Choice
- Supplements
- E-Collections
- Virtual Roundtables
- Author Videos
- Author Guidelines
- Submission Site
- Open Access Options
- About The European Journal of Public Health
- About the European Public Health Association
- Editorial Board
- Advertising and Corporate Services
- Journals Career Network
- Self-Archiving Policy
- Terms and Conditions
- Explore Publishing with EJPH
- Journals on Oxford Academic
- Books on Oxford Academic

Article Contents
- < Previous
Why do we need for timeliness of research in decision-making?
- Article contents
- Figures & tables
- Supplementary Data
J de Jong, J Hansen, P Groenewegen, Why do we need for timeliness of research in decision-making?, European Journal of Public Health , Volume 29, Issue Supplement_4, November 2019, ckz185.216, https://doi.org/10.1093/eurpub/ckz185.216
- Permissions Icon Permissions
Compared to the policy process, the research process is slow. As a result, research evidence is not always available when needed in the policy process. These differences in timelines between research and policy hinder the use of research evidence in the policy process. In order to support evidence-based policy making, timeliness of research is important.
Examples are provided, e.g. where research was on time to be included in the policy process and where research was too late to be included in it. These examples are described and analysed to provide for recommendations on how to better align both processes.
It is shown that in order to create timeliness of research, policy makers and researchers should talk on a regular basis. This increases the chance that results from the research are included in policy making.
Timeliness of research is important for evidence-based policy making. In order to create timeliness of research, interaction between researchers and policy makers is important.
- decision making
- policy making
- evidence-based practice
| Month: | Total Views: |
|---|---|
| November 2019 | 3 |
| December 2019 | 1 |
| February 2020 | 1 |
| March 2020 | 1 |
| April 2020 | 1 |
| June 2020 | 3 |
| July 2020 | 3 |
| August 2020 | 8 |
| September 2020 | 6 |
| October 2020 | 6 |
| November 2020 | 7 |
| December 2020 | 12 |
| January 2021 | 12 |
| February 2021 | 16 |
| March 2021 | 14 |
| April 2021 | 33 |
| May 2021 | 23 |
| June 2021 | 16 |
| July 2021 | 17 |
| August 2021 | 7 |
| September 2021 | 20 |
| October 2021 | 21 |
| November 2021 | 20 |
| December 2021 | 15 |
| January 2022 | 15 |
| February 2022 | 13 |
| March 2022 | 24 |
| April 2022 | 18 |
| May 2022 | 25 |
| June 2022 | 22 |
| July 2022 | 11 |
| August 2022 | 9 |
| September 2022 | 18 |
| October 2022 | 15 |
| November 2022 | 18 |
| December 2022 | 10 |
| January 2023 | 25 |
| February 2023 | 14 |
| March 2023 | 17 |
| April 2023 | 25 |
| May 2023 | 27 |
| June 2023 | 16 |
| July 2023 | 17 |
| August 2023 | 12 |
| September 2023 | 5 |
| October 2023 | 16 |
| November 2023 | 12 |
| December 2023 | 12 |
| January 2024 | 14 |
| February 2024 | 22 |
| March 2024 | 27 |
| April 2024 | 21 |
| May 2024 | 19 |
| June 2024 | 12 |
| July 2024 | 1 |
Email alerts
Citing articles via.
- Contact EUPHA
- Recommend to your Library
Affiliations
- Online ISSN 1464-360X
- Print ISSN 1101-1262
- Copyright © 2024 European Public Health Association
- About Oxford Academic
- Publish journals with us
- University press partners
- What we publish
- New features
- Open access
- Institutional account management
- Rights and permissions
- Get help with access
- Accessibility
- Advertising
- Media enquiries
- Oxford University Press
- Oxford Languages
- University of Oxford
Oxford University Press is a department of the University of Oxford. It furthers the University's objective of excellence in research, scholarship, and education by publishing worldwide
- Copyright © 2024 Oxford University Press
- Cookie settings
- Cookie policy
- Privacy policy
- Legal notice
This Feature Is Available To Subscribers Only
Sign In or Create an Account
This PDF is available to Subscribers Only
For full access to this pdf, sign in to an existing account, or purchase an annual subscription.
- Research article
- Open access
- Published: 25 November 2017
Is the information of systematic reviews published in nursing journals up-to-date? a cross-sectional study
- Wilson W. S. Tam 1 ,
- Kenneth K. H. Lo 2 ,
- Parames Khalechelvam 1 ,
- Joey Seah 1 &
- Shawn Y. S. Goh 1
BMC Medical Research Methodology volume 17 , Article number: 151 ( 2017 ) Cite this article
9135 Accesses
16 Citations
11 Altmetric
Metrics details
An up-to-date systematic review is important for researchers to decide whether to embark on new research or continue supporting ongoing studies. The aim of this study is to examine the time taken between the last search, submission, acceptance and publication dates of systematic reviews published in nursing journals.
Nursing journals indexed in Journal Citation Reports were first identified. Thereafter, systematic reviews published in these journals in 2014 were extracted from three databases. The quality of the systematic reviews were evaluated by the AMSTAR. The last search, submission, acceptance, online publication, full publication dates and other characteristics of the systematic reviews were recorded. The time taken between the five dates was then computed. Descriptive statistics were used to summarize the time differences; non-parametric statistics were used to examine the association between the time taken from the last search and full publication alongside other potential factors, including the funding support, submission during holiday periods, number of records retrieved from database, inclusion of meta-analysis, and quality of the review.
A total of 107 nursing journals were included in this study, from which 1070 articles were identified through the database search. After screening for eligibility, 202 systematic reviews were included in the analysis. The quality of these reviews was low with the median score of 3 out of 11. A total of 172 (85.1%), 72 (35.6%), 153 (75.7%) and 149 (73.8%) systematic reviews provided their last search, submission, acceptance and online published dates respectively. The median numbers of days taken from the last search to acceptance and to full publication were, respectively, 393 (IQR: 212–609) and 669 (427–915) whereas that from submission to full publication was 365 (243–486). Moreover, the median number of days from the last search to submission and from submission to online publication were 167.5 (53.5–427) and 153 (92–212), respectively. No significant association were revealed between the time lag and those potential factors.
The median time from the last search to acceptance for systematic reviews published in nursing journals was 393 days. Readers for systematic reviews are advised to check the time taken from the last search date of the reviews in order to ensure that up-to-date evidence is consulted for effective clinical decision-making.
Peer Review reports
A systematic review (SR) refers to secondary research that not only systematically synthesizes all available research evidence relevant to a particular topic, but also interprets, evaluates and appraises the quality of such results [ 1 ]. With up-to-date results from SRs, relevant evidence becomes available for researchers to decide not only whether to embark on new research but also whether to continue supporting ongoing studies [ 2 , 3 ]. Many policymakers and stakeholders seek to use research evidence to influence policymaking, for whom systematic reviews have become an indispensable resources. [ 4 ] With the dynamic nature of gathering and presenting research evidence, SRs must be up-to-date to enable different stakeholders such as researchers, funding bodies, and data-monitoring committees, to use reliable evidence to inform decision-making [ 2 ].
Against this background, it is therefore important to ascertain whether the information published in the SRs are up-to-date. In their evaluation of 300 SRs published in Core Clinical Journals, Beller et al. [ 5 ] found that the median time from the last search date to first publication was 8 months (~240 days). Another study reported that the median time taken for a research article published in top nursing journals from the end of data collection to first publication was 855 days [ 6 ]. However, an interesting gap to explore has remained in the literature: no studies have been conducted to specifically examine the time lag for SRs published in nursing journals.
SRs with longer time lags of publication may appear to be less convincing for the stakeholders due to the concern with less updated evidence. However, such impact on decision-making also depends on the frequency of publication of primary studies in the topic. For example, if multiple new studies are published every year, one or 2 years’ delay in publishing the SR will imply the untimely exclusion of such newly published studies; otherwise, there is less impact of delayed publication on the timeliness of findings. A recently published meta-epidemiological study [ 7 ] reported that 73% of the SRs published in top medical journals included 10 or more studies while Pollkki et al. [ 8 ] reported a median of 15 studies were included among 39 SRs in high-impact nursing journals. Nevertheless, they did not examine the average number of those studies by the years of the SRs.
The time taken for completing the SRs also affects the time required for publication. Problem identification, search-strategy development, database search, study selection, data extraction, data analysis and synthesis are the basic steps in conducting systematic reviews. Intuitively, if copious records are retrieved from database, more time is expected for study selection and data extraction; therefore, the number of records retrieved may relate to the time taken for publication. Furthermore, performing meta-analysis requires specific training but it has been reported that many nursing researchers and students did not fully understand the statistical techniques of meta-analysis or the various important concepts that underpin it [ 9 ]. Thus, the inclusion of meta-analyses in the SR may take more time to complete the review.
Another aspect to influence the speed of publication is the journal review process. Publishing a SR in a peer-reviewed journal usually involves several phases including manuscript submission, first decisions from editors, peer-reviews, follow-up decisions from the editors, and revision and re-submission. The whole process can be repeated numerous times if the SR is rejected at the editor’s first decision, thereby prolonging the publication process: it has been suggested that editors of nursing journals would take at least 8 weeks to first decide whether to accept a manuscript, or to request revisions [ 10 ]. In addition, the timing of submission has been suggested to affect the time taken for the peer-reviews as it would be difficult for editors to recruit peer-reviewers during holiday periods [ 11 ]. No studies have hitherto examined these effects in the publication process of SRs but they are clearly critical.
On the other hand, the methodological quality of SRs plays an important role in drawing conclusions on intervention effectiveness and carries implications for clinical decision-making. [ 12 ] Although studies have examined the methodological quality of SRs [ 8 , 13 , 14 , 15 ], none of them have examined the association between the quality and the time taken for publication. Besides, Gomez-Garcia et al. [ 16 ] reported that funding from academic institutions was associated with a higher quality of SRs and hence the funding sources may also affect the time lag.
Given the aforementioned uncertainties, the primary aim of this study is to evaluate the timeliness of SRs published in nursing journals upon first publication, as measured by the time taken from the last search date to actual publication. The total time taken was divided into stages, including the time from the last search dates to the acceptance, online publication, or full publication. The secondary aim is to explore the factors potentially associated with the time taken, such as study quality, funding source, number of submission, et cetera.
Study design
A cross-sectional study was conducted to examine the time taken from the last search date to actual publication of SRs in nursing journals. The SRs were extracted from three scholarly databases in 2014.
Inclusion and exclusion criteria
Articles included in this study are self-proclaimed SRs, systematic literature reviews or those that included the term “meta-analyses” in the title, abstract, or both. Only SRs in English were included. Methodological papers, commentaries, conference abstracts, or letters on SRs or meta-analyses were excluded.
Search strategy
Nursing journals were first identified from the category of “Nursing Studies” within the 2013 edition for Journal Citation Reports (Science) as this was the latest available version in early 2015. This approach has been widely used to identify journal titles for a specific field in citation analysis [ 17 , 18 ]. A search, involving combinations of journal titles and keywords, was then conducted to identify the SRs from three databases, namely, Cumulative Index of Nursing and Allied Health Literature (CINAHL), PubMed, and Web of Science. The keyword search included “systematic review,” “meta*analys*,” or “pooled analysis*”, were adopted to identify SRs and meta-analyses in other studies [ 19 , 20 ]. Only SRs published in 2014 were included based on their full publication date (with volume and page numbers) as this study was concluded in 2015. The results from each database were then imported to EndNote X7 with duplicate records removed. The final search was conducted in May 2015. The SRs were originally identified for another study [ 20 ].
Selection of articles
The titles and abstracts of the articles were screened by two independent reviewers (KL and PK) to identify the SRs for inclusion. Full texts of all potential articles were then downloaded for further evaluation. Any discrepancies between the two reviewers were resolved by reaching a consensus. When incongruities persisted, a third reviewer (WT) was consulted to confirm the final inclusion.
Data extraction
Data of the SRs, including the first author’s name, title, journal name, number of pages, inclusion of meta-analysis, funding source, and other information, were extracted by two independent reviewers (WT and PK). WT and SG then classified the SRs according to the four scopes (Clinical Research, Health Systems and Outcomes Research, Nursing Education Research, and Others) as suggested by the American Association of College of Nursing [ 21 ]. Dates of full publication, online publication, acceptance and submission of the included SRs were extracted from the databases, journal homepages, or both. If only the month or months, such as March or March to April, were available, then the first date of the period was used as the date (i.e., March 1st). The last search date of each SR was extracted from the full text. If only the year was specified, then the mid-year (i.e., June 1st) was used as the search end date. The differences (in days) between the last search date and (i) publication date, (ii) online publication date, and (iii) acceptance date were computed for each SR. We also contacted the corresponding author of each included SR by e-mail to investigate the number of journals to which he or she submitted before the SR was accepted for publication.
Quality assessment
The methodological quality of the included SRs was assessed by A Measurement Tool to Assess Systematic Reviews (AMSTAR), a validated checklist comprising 11 items addressing important aspects of SRs such as the availability of protocols, use of independent reviewers, comprehensiveness of databases, exploration of grey literature, and quality assessment of included studies. [ 12 , 22 ]. Each of the checklist items was scored “Yes”, “No”, “Cannot Answer” or “Not Applicable” (NA). A higher number of items assigned “Yes”, signifies a superior methodological quality of the reviews. The assessment was conducted by two authors independently (WT and JS), who subsequently resolved any discrepancies by consensus. The number of “Yes” for each item was counted for each review. An overall score of 4 or less represented poor methodological quality, 5 to 8 was considered fair to good, and 9 or greater was deemed to be good [ 23 ].
Data analysis
Descriptive statistics, including the median, inter-quartile range (IQR), frequency, and percentages, were used to summarize the characteristics of the included SRs. The median and IQR were then computed for the differences in all included studies. The Mann-Whitney U or Kruskal-Wallis test was used to examine whether the time from last search to full publication varied by different characteristics including the quality of the SRs, availability of funding support, holiday period, and number of records identified in database search. All analyses were conducted using IBM SPSS statistics 24, while the PRISMA flowchart was generated using PRISMA Flow Diagram Generator [ 24 ].
A total of 107 journals were identified from the Journal Citation Reports (see Additional file 1 : Table S1 for the list of journals with the hyperlinks to their homepages), from which 1070 articles were identified during the database search. Upon removal of duplicate articles and those from non-nursing journals (e.g., Heart and Lung belonged to nursing journals whereas Heart, Lung and Circulation did not), 949 articles were screened and evaluated through their title and abstract for eligibility. Following this, 243 potential articles were identified; however, 41 were excluded as they were either duplicates (12) or the full text was not written in English or the paper had no full text (29), leaving 202 SRs in this study. Figure 1 depicts the flow of SR selection.
PRISMA flowchart. The diagram was generated using PRISMA Flow Diagram Generator by Toronto Health Economics and Technology Assessment Collaboration ( http://prisma.thetacollaborative.ca /)
Characteristics of the 202 systematic reviews
Table 1 summarizes the characteristics of the 202 SRs, the full list for which is in the Additional file 2 : Table S2. Among the SRs, 59 (29.2%), 53 (26.2%), 36 (17.8%), and 54 (26.7%) were published in the first, second, third, and fourth quarters of 2014, respectively. These SRs were published in 71 nursing journals, and the median number of SRs published in each journal was 2 (IQR: 1–3). More than 10 SRs were published in four journals in 2014, i.e., International Journal of Nursing Studies , Journal of Clinical Nursing , Journal of Advanced Nursing , and Worldviews of Evidence-Based Nursing . The scopes of the SRs were classified into four groups, i.e. Clinical Research ( n = 145, 71.8%), Health Systems and Outcomes Research ( n = 30, 14.9%), Nursing Education Research ( n = 20, 9.9%), and Others ( n = 7, 3.5%). A total of 172 (85.1%), 72 (35.6%), 153 (75.7%) and 149 (73.8%) of the SRs provided, respectively, dates of the last search, submission, acceptance and online publication. In addition, 198 (98.0%) of the SRs stated the databases used for the search, 37 (18.3%) included meta-analyses, and 108 (53.5%) disclosed the funding information.
We attempted to contact the corresponding authors by e-mails for additional information but no e-mail addresses were provided in 13 papers. Therefore, a total of 189 e-mails were sent but 30 e-mail addresses were no longer valid. Among the 159 valid e-mail addresses, we received replies from 62 authors (response rate ~39.0%). Of them, 47 (75.8%) clarified that the journals were their first attempts while 10 (16.1%) clarified that they were their second attempts.
The methodological quality measured by the AMSTAR is summarized in Table 2 . The median number of “Yes” obtained by the SRs was 3 (IQR: 2–5). A total of 139 (68.8%) SRs were classified as poor quality. For individual items, the percentage of “Yes” ranged from 0.0% (item 11) to 83.2% (item 6).
The median (IQR) numbers of days taken from the last search to acceptance, to online publication, and to full publication of the SRs are 393 (212–609), 455 (273–654.5), and 669 (IQR: 427–915), respectively (Table 3 ). Secondly, the median (IQR) numbers of days from submission to acceptance, to online publication and to full publication were 153 (92–212), 212 (151–243) and 365 (243–486), respectively. However, it is noteworthy that only 72 SRs, around one-third of all included, provided their submission dates, thereby possibly rendering the results inaccurate. Lastly, the median (IQR) duration from acceptance to online publication was 59 (30–92) days, while that from online publication to full publication was 242 (153–365) days.
No significant difference was observed in the time from last search to acceptance and to full publication (Table 4 ), with respect to factors such as the availability of the funding, holiday period submission, number of records identified in databases, and quality of studies.
The identification of comprehensive and up-to-date SRs is important for researchers when evaluating evidence relevant to their topic of interest [ 25 ]. Our results revealed that the median time taken from the last search date to the online and full publication for the SRs in nursing journals were 455 and 669 days. These duration are markedly longer than those in medical journals (i.e., an average of 5.1 months from last search to first publication) [ 5 ]. The lack of timeliness in this context may jeopardize end-users such as guideline producers or policy makers in developing guidelines or revising policies as up-to-dated information may be missed.
In our study, the median time from the last search date to publication was 669 days (i.e., approximately 22.3 months). It has been advocated that systematic reviewers should update their literature search biennially to determine new studies for inclusion into a previously completed SR for updating of evidence [ 26 ]. Therefore, the time taken for publishing SRs in nursing journals is considered excessively long. Such time lags can actually be classified into three categories: from the last search date to submission, from submission to acceptance, and from acceptance to online publication.
The median time from the last search date to acceptance in nursing journals was 393 days, approximately 2.5-fold longer than those in Core Clinical Journals (5.1 months or approximately 153 days) [ 5 ]. The time taken can be classified into two periods: from the last search date to submission and from submission to acceptance. From our results, the median time from the last search date to submission was 167.5 days. The time taken was expended on the authors’ preparation of the manuscript and attempts of submission to journals. According to Polit and Beck [ 27 ], in conducting a SR, five steps are warranted after the literature search, i.e. selecting the studies, evaluating study quality, extracting and encoding data, analyzing and interpreting data (i.e., meta-analysis or synthesis), and writing the review. The time taken to complete these steps varies as this may depend on the researchers’ experiences. Therefore, having an experienced systematic reviewer within the authoring team may expedite these steps. For example, to register a new review with Cochrane Collaboration, a requirement is that at least one author must possess the experience in completing at least one Cochrane Review [ 28 ]. This requirement ensures the timeliness and quality of the review process.
In addition, authors are suggested to conduct preliminary selection of appropriate journals, from which the resultant review will more likely be accepted. This will avoid delays caused by multiple attempts when submitting to different journals [ 29 , 30 ]. We contacted the corresponding authors of the 202 reviews and received replies from 62 authors, of whom 47 (75.8%) clarified that their papers were published in the journal in their first attempt. Therefore, such an effect should not be a critical factor among the SRs. However, as the SRs should be submitted before 2014, recall bias from the authors could not be ruled out.
The median time taken for SRs from submission to acceptance was found to be 153 days in this study. It includes the time for review and revision of the submitted manuscript. In comparison, the average time from submission to acceptance for journals from different disciplines was around 6.41 months (~192 days), which is longer than our result [ 31 ]. Some common problems identified for the delays in the review process include discrepancies with journal guidelines, submission during peak periods, reviewers’ delays, and failure to address reviewers’ comments or not submitting revisions on time [ 11 ]. For each of these problems, solutions are suggested to avoid unnecessary delays. As regards discrepancies with journal guidelines, although most authors adhere to the guidelines of the journals, when their manuscript is rejected by one journal, they may directly send the rejected manuscript to another without making any necessary changes. Further delays may follow when the editorial office of the second journal realizes stylistic and guideline breaches of the unedited manuscript and, in rejection, return it to the authors [ 32 ].
Some suggested that manuscript submission during holiday periods would probably lengthen the review process. There appears to be a propensity among some researchers to make use of the holiday to finalize and submit their manuscripts. Nevertheless, during this period, journal editors will find it difficult in recruiting potential reviewers, as some may be on vacation. [ 11 ]. However, no such observation can be concluded from our findings.
Reviewers’ delays may be resolved by shortening the timeframe for review. According to a recent study, some journals do not provide any deadline for their reviewers, whereas others allow up to 1 year [ 33 ]. In the same study, an experiment was conducted where all the participating journals were requested to shorten their current imposed review period by a minimum of 1 week. The results revealed a reduction in the editing time by at least 1 week on average, with several participating journals improving by more than 2 months [ 33 ]. In addition, the study revealed that reviewers were more likely to accept invitations with a shorter response timeframe [ 33 ].
The last problem concerns authors’ failures to address reviewers’ comments or not submitting revisions on time. The time estimated for nursing journals to complete the review is at least 8 weeks, when the editor will then make the first decision to accept or reject the manuscript, or to request revisions [ 10 ]. After receiving comments from the editor and reviewers, the authors should adequately address their comments by highlighting any changes in the manuscript and drafting a point-to-point response letter to expedite decision [ 10 ]. In addition, the authors should adhere to the deadline set by the journals to avoid their manuscripts being treated as new submissions or facing new reviewers [ 11 ]. The aforementioned strategies may collectively mitigate the four potential problems underlying excessive delays and thereby shorten the time taken from the last search date to the acceptance date. From the perspective of the journal editors, they may consider emulating the practice of Cochrane Database of Systematic Reviews where an updated literature search is required if the initial search was conducted more than 6 months prior to the review of the manuscript, as has been adopted by some General Medical Journals such as Annals of Internal Medicine . This will lessen the time lag between the search and the SR publication. Unless such an updated search before acceptance is made compulsory by journals, it is probable that some authors will not prioritize it since their results and, by extension, the discussion and conclusion may change.
The median time taken from acceptance to online publication of SRs published in nursing journals was 59 days. Such a duration may admittedly not be considered long but this is in fact twice the median time taken compared with papers found on PUBMED 2014 (approximately 25 days) [ 34 ]. This timing varies among different publishers and with current technology the situation should improve. The median time taken from online publication to full publication was 212 days (approximately 7 months). One possible reason underlying the time lags is the overwhelming number of accepted articles that is not commensurate with the publishing space in the journals. Nevertheless, this issue may become less critical with the increasing availability of the online early views in many journals for readers. Our results show that 149 (73.8%) SRs indicated their online publication dates; hence, it may be concluded that at least 73.8% of the SRs were made available earlier than the full publication date. Our results also suggest that the average time taken from acceptance to publication is 242 days. This is considered an improvement compared with the circumstance 10 years ago when the publication of SRs would usually take more than a year in most nursing journals [ 35 ].
According to Item 7 in the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines, authors of SRs should include all information sources (e.g., databases with dates of coverage, and the search and last search dates) [ 36 ]. Among the 202 SRs identified, 172 (85.1%) provided the last search date, which is slightly lower than Core Clinical Journals (90.3%) [ 5 ]. An overwhelming majority numbering 198 (98.0%) of the identified SRs stated the databases used for their search. This is comparable with the figure previously reported (98.3%) by Beller et al. [ 5 ]. Against this background, Liberati et al. [ 37 ] further suggested that this information would allow researchers to assess the scientific value of the review as the publication time lags may necessitate updates of SRs by the respective authors.
The quality of our included SRs was in general low with a median score of 3 out of 11. It is lower than the journals in Orthodontic (with mean scores 3.5 to 5.66) [ 23 ] or Pain related SRs (median: 6; IQR: 4–7) [ 13 ]. Two potential reasons underlie this low quality, the first of which concerns the lack of adherence among the authors to the PRISMA guideline in their reviews. Only 30 out of the 107 journals mandated the use of the PRISMA guideline [ 20 ]; accordingly, there might have been inadvertent omission of information in reporting their results. For example, the independent selection of papers might have been performed but this might not be reflected in the published review. The other potential reason concerns our stringent conformance to the AMSTAR criteria in examining the methodological quality. The generally low quality of our included SRs might be attributed to some AMSTAR criteria that were unfeasibly difficult to fulfill: for example, the last item on the AMSTAR checklist – “ Was the conflict of interest included? ” – requests the authors to indicate all sources of funding or support for the SRs and each of the studies included therein. The compliance to this item was often low and has indeed been reported to be approximately only 10% in the field of pain research [ 13 ]. Some studies would remove this item in evaluating the quality of SRs [ 38 ] whereas others would (more leniently) consider the disclosure of funding only for the authors but not for the individual studies included in the SRs [ 39 ]. Such refinements of definitions of the AMSTAR criteria may lead to a higher quality for the included studies.
Strength and limitations
To the best of our knowledge, this is the first study focusing on the publication time lags of SRs published in nursing journals. The study sample is reasonably large with 202 SRs. Robust procedures have been adopted such as independent data extraction and evaluation, to ensure the accuracy of the results. Nevertheless, certain limitations of this study deserve attention. Firstly, only SRs published in 2014 were included as this study was conducted primarily in 2015 when 2014 was then the latest available full year. We did not include any preceding years because of limited resources but we believe that the observed pattern would be similar for 2015 or 2016. Secondly, the methodological quality of the SRs was generally low. Thirdly, non-English SRs were excluded due to language barriers of the authors; however, the time taken is expected to be similar or even longer. Fourthly, as a database search was used to identify the SRs, the possibility cannot be discounted that some articles might be missed if they had not included any words related to SR or mete-analysis. However, this method is considered acceptable. Fifthly, although the authors were contacted for additional information, only 2 questions were posted by e-mail to ensure an acceptable response rate. Further studies are recommended to explore the topic from both the journal editors’ and authors’ perspectives. Finally, given the absence of submission dates of most SRs, further analysis could not be conducted for most of them.
Our study revealed a median difference of 669 days (approximately 22.3 months) between the last search date and the full publication date. With this information, journals should consider requesting authors of SRs to update their literature search before the acceptance of the SRs. SR users should also ascertain the time lag between the last search date of the reviews to ensure that the evidence is up-to-date for effective clinical decision-making.
Glasziou P, Irwig L, Bain C, Colditz G: Systematic reviews in health care a practical guide. In . Cambridge: Cambridge University Press,; 2001: 1 online resource (148 p.).
Chalmers I. Chapter 24: using systematic reviews and registers of ongoing trials for scientific and ethical trial design, monitoring, and reporting. In: Egger M, Smith GD, Altman DG, editors. Systematic reviews in health care : meta-analysis in context. 2nd ed. London: BMJ; 2001. p. 429–43.
Chapter Google Scholar
Sutton AJ, Cooper NJ, Jones DR. Evidence synthesis as the key to more coherent and efficient research. BMC Med Res Methodol. 2009;9:29.
Article PubMed PubMed Central Google Scholar
Lavis JN. How can we support the use of systematic reviews in policymaking? PLoS Med. 2009;6(11):e1000141.
Beller EM, Chen JK, Wang UL, Glasziou PP. Are systematic reviews up-to-date at the time of publication? Syst Rev. 2013;2:36.
Palese A, Coletti S, Dante A. Publication efficiency among the higher impact factor nursing journals in 2009: a retrospective analysis. Int J Nurs Stud. 2013;50(4):543–51.
Article PubMed Google Scholar
Tsujimoto Y, Tsujimoto H, Kataoka Y, Kimachi M, Shimizu S, Ikenoue T, Fukuma S, Yamamoto Y, Fukuhara S. Majority of systematic reviews published in high-impact journals neglected to register the protocols: a meta-epidemiological study. J Clin Epidemiol. 2017;84:54–60.
Polkki T, Kanste O, Kaariainen M, Elo S, Kyngas H. The methodological quality of systematic reviews published in high-impact nursing journals: a review of the literature. J Clin Nurs. 2014;23(3–4):315–32.
Bath-Hextall F, Wharrad H, Leonardi-Bee J. Teaching tools in evidence based practice: evaluation of reusable learning objects (RLOs) for learning about meta-analysis. BMC Med Educ. 2011;11:18.
Oermann MH. Chapter 13: editorial review process. In: Writing for publication in nursing. Philadelphia: Lippincott; 2002. p. 249–73.
Google Scholar
Davidhizar R, Bechtel GA. Avoiding publication delays: author and editor responsibilities. Nurse Author Ed. 1999;9(4):1–4. 7
CAS PubMed Google Scholar
Shea BJ, Hamel C, Wells GA, Bouter LM, Kristjansson E, Grimshaw J, Henry DA, Boers M. AMSTAR is a reliable and valid measurement tool to assess the methodological quality of systematic reviews. J Clin Epidemiol. 2009;62(10):1013–20.
Riado Minguez D, Kowalski M, Vallve Odena M, Longin Pontzen D, Jelicic Kadic A, Jeric M, Dosenovic S, Jakus D, Vrdoljak M, Poklepovic Pericic T, et al. Methodological and reporting quality of systematic reviews published in the highest ranking journals in the field of pain. Anesth Analg. 2017;
Samargandi OA, Hasan H. The quality of systematic reviews in hand surgery: an analysis using AMSTAR. Plast Reconstr Surg. 2014;134(3):482e–3e.
Article CAS PubMed Google Scholar
Sequeira-Byron P, Fedorowicz Z, Jagannath VA, Sharif MO. An AMSTAR assessment of the methodological quality of systematic reviews of oral healthcare interventions published in the journal of applied oral science (JAOS). J Appl Oral Sci. 2011;19(5):440–7.
Gomez-Garcia F, Ruano J, Aguilar-Luque M, Gay-Mimbrera J, Maestre-Lopez B, Sanz-Cabanillas JL, Carmona-Fernandez PJ, Gonzalez-Padilla M, Velez Garcia-Nieto A, Isla-Tejera B. Systematic reviews and meta-analyses on psoriasis: role of funding sources, conflict of interest and bibliometric indices as predictors of methodological quality. Br J Dermatol. 2017;176(6):1633–44.
Brandt JS, Downing AC, Howard DL, Kofinas JD, Chasen ST. Citation classics in obstetrics and gynecology: the 100 most frequently cited journal articles in the last 50 years. Am J Obstet Gynecol. 2010;203(4):355.e1–7.
Article Google Scholar
Tam WW, Wong EL, Wong FC, Hui DS. Citation classics: top 50 cited articles in 'respiratory system'. Respirology. 2013;18(1):71–81.
Huang Y, Mao C, Yuan J, Yang Z, Di M, Tam WW, Tang J. Distribution and epidemiological characteristics of published individual patient data meta-analyses. PLoS One. 2014;9(6):e100151.
Tam WWS, Lo KKH. Khalechelvam P: Endorsement of PRISMA statement and quality of systematic reviews and meta-analyses published in nursing journals: a cross-sectional study. BMJ Open. 2017;7(2):e013905.
Nursing Research, American Association of Colleges of Nursing. http://www.aacnnursing.org/News-Information/Position-Statements-White-Papers/Nursing-Research .
Shea BJ, Bouter LM, Peterson J, Boers M, Andersson N, Ortiz Z, Ramsay T, Bai A, Shukla VK, Grimshaw JM. External validation of a measurement tool to assess systematic reviews (AMSTAR). PLoS One. 2007;2(12):e1350.
Fleming PS, Seehra J, Polychronopoulou A, Fedorowicz Z, Pandis N. Cochrane and non-Cochrane systematic reviews in leading orthodontic journals: a quality paradigm? Eur J Orthod. 2013;35(2):244–8.
THETA: PRISMA flow diagram generator. In: Toronto health economics and technology assessment (THETA) collaboration . Edited by Collaboration THEaTAT. Canada: Toronto Health Economics and Technology Assessment (THETA) Collaboration; 2016.
Evans D. Systematic reviews of nursing research. Intensive Crit Care Nurs. 2001;17(1):51–7.
Moher D, Tsertsvadze A, Tricco AC, Eccles M, Grimshaw J, Sampson M, Barrowman N. When and how to update systematic reviews. Cochrane Database Syst Rev. 2008;1:MR000023.
Polit DF, Beck CT. Chaptaer 27: systematic reviews of research evidence: Metaanalysis, Metasynthesis, and mixed studies review. In: Nursing research : generating and assessing evidence for nursing practice. Ninth ed. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2012. p. xiv, 802 pages.
Resources, Cochrane Pregnancy and Childbirth Group, Cochrane Collaboration. http://pregnancy.cochrane.org/resources .
Shojania KG, Sampson M, Ansari MT, Ji J, Doucette S, Moher D. How quickly do systematic reviews go out of date? A survival analysis. Ann Intern Med. 2007;147(4):224–33.
Welch SJ. Selecting the right journal for your submission. J Thorac Dis. 2012;4(3):336–8.
PubMed PubMed Central Google Scholar
Björka B, Soloman D. The publishing delay in scholarly peer-reviewed journals. J Informetrics. 2013;7(4):10.
Guide for Authors: The Journal of Allergy and Clinical Immunology.
Leeuwendal A. Elsevier initiative leads to faster revision and review times: Shorter lead-in times for reviews and author revisions result in articles appearing online more quickly. Posted on 11 May 2015. https://www.elsevier.com/reviewers-update/story/innovation-in-publishing/elsevier-initiative-leads-to-fasterrevision-and-review-times .
Powell K. Does it take too long to publish research? Nature. 2016;530:3.
Parahoo K. Chapter 7: literature reviews. In: Parahoo K, editor. Nursing research : principles, process and issues. 2nd ed. Basingstoke England: New York: Palgrave Macmillan; 2014. p. xii, 440 p.
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6(7):e1000100.
Panic N, Leoncini E, de Belvis G, Ricciardi W, Boccia S. Evaluation of the endorsement of the preferred reporting items for systematic reviews and meta-analysis (PRISMA) statement on the quality of published systematic review and meta-analyses. PLoS One. 2013;8(12):e83138.
Seo HJ, Kim KU. Quality assessment of systematic reviews or meta-analyses of nursing interventions conducted by Korean reviewers. BMC Med Res Methodol. 2012;12:129.
Download references
Acknowledgements
We would like to thank the corresponding authors of the included reviews for replying our e-mails.
The study has partly been supported by the University Start-up Grant of the first author WT (Ref. No.: NUHSRO/2014/101/SU/01).
The funding body has played no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Availability of data and materials
All data generated or analyzed in this study were extracted from published systematic reviews [The systematic reviews are listed in the supplementary file].
Author information
Authors and affiliations.
Alice Lee Centre for Nursing Studies, Yong Loo Lin School of Medicine, Level 2, Clinical Research Centre, Block MD11, 10 Medical Drive, Singapore, 117597, Singapore
Wilson W. S. Tam, Parames Khalechelvam, Joey Seah & Shawn Y. S. Goh
4/F, JC School of Public Health and Primary Care, The Chinese University of Hong Kong, Shatin, HKSAR, Hong Kong
Kenneth K. H. Lo
You can also search for this author in PubMed Google Scholar
Contributions
WT & KL designed the study; WT, KL & PK identified the systematic reviews; WT, PK, JS & SG extracted the data; WT, KL & JS conducted the analysis; WT, KL & SG drafted the manuscript. All authors read and approved the final manuscript.
Corresponding author
Correspondence to Wilson W. S. Tam .
Ethics declarations
Ethics approval and consent to participate.
Not applicable.
Consent for publication
Competing interests.
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1: table s1..
Full list of journals indexed in Journal Citation Reports (Science Edition). (DOCX 24 kb)
Additional file 2: Table S2.
Full list of included articles in this study. (DOCX 41 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License ( http://creativecommons.org/licenses/by/4.0/ ), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated.
Reprints and permissions
About this article
Cite this article.
Tam, W.W.S., Lo, K.K.H., Khalechelvam, P. et al. Is the information of systematic reviews published in nursing journals up-to-date? a cross-sectional study. BMC Med Res Methodol 17 , 151 (2017). https://doi.org/10.1186/s12874-017-0432-3
Download citation
Received : 27 July 2017
Accepted : 16 November 2017
Published : 25 November 2017
DOI : https://doi.org/10.1186/s12874-017-0432-3
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Systematic reviews
- Quality of reporting
- Information retrieval
- Presentation and publication policy
- Evidence-based nursing
BMC Medical Research Methodology
ISSN: 1471-2288
- General enquiries: [email protected]
- Research and Innovation
- The Abstract
- Audio Abstract Podcast
- Centennial Campus
- Campus Life
- Faculty and Staff
- Awards and Honors
- HR and Finance
- Resilient Pack
- We Are the Wolfpack
- Service and Community
- Red Chair Chats
- News Releases
- In the News
- NC State Experts on 2024 Elections
- NC State Experts Available on Climate
- NC State Experts on Roe v. Wade
- NC State Supply Chain Experts
- Experts on COVID-19
- Hurricane Experts
- About NC State News
- Faculty Support
- Training Program
Fires and Climate are Changing. Science Needs to Change too.

A new white paper on the many ways wildfires affect people and the planet makes clear that as fires become more intense and frequent, the urgency for effective and proactive fire science grows. By addressing these challenges, the fire research community aims to better protect our planet and its inhabitants.
Fire is a natural part of life on Earth, sustaining healthy and balanced ecosystems worldwide. But human activity and a changing climate are rapidly shifting both the frequency and severity of wildfire events, creating new risks to human and environmental health.
Recently, a group of scientists from 14 countries and across several disciplines – physical and social sciences, mathematics, statistics, remote sensing, fire communication and art, operational fire science, and fire management – gathered to discuss rapid changes in fire regimes and identify pathways to address these challenges.
The experts identified three grand challenges for fire science in the coming decades: understanding the role of fire in the carbon cycle, fire and extreme events, and the role of humans in fire.
“If we want to improve the assessment of future fire impacts on people and the planet, we need to start with a better understanding of how climate, land cover changes, and human land management practices drive fire distribution and severity in the coming decades,” says Douglas Hamilton, assistant professor of marine, earth and atmospheric science at North Carolina State University.
Hamilton, together with Morgane Perron of University Brest, France and Joan Llort of the Barcelona Supercomputing Centre, Spain, initiated the working group FLARE (which stands for Fire Science Learning AcRoss the Earth System).
To address the grand challenges, the scientists identified three pressing research priorities: understanding the net carbon balance of fire, developing rapid response tools for wildfire events, and understanding fire’s impact on society, especially marginalized and underrepresented populations.
The first priority, understanding the net carbon balance of fire, refers to understanding how fire’s carbon release, ecological recovery from fire, climate change, ocean biology, and ice melt all interact and affect the Earth’s carbon balance.
“Wildfires can significantly affect the global carbon cycle,” says Chantelle Burton, senior climate scientist at the Met Office UK. “Fires in ecosystems that store large amounts of carbon, such as peatlands, permafrost and forests, can release vast quantities of CO2 into the atmosphere. However, where that carbon ultimately ends up and its impact on future warming are harder to determine. Incorporating accurate fire-related carbon fluxes into Earth System Models is crucial for predicting climate outcomes and informing mitigation strategies, and it will require us to bring together experts from across the fire sciences.”
The second priority, developing rapid response tools for wildfire events, refers to developing tools for more timely and responsive answers to critical questions during extreme fire events and providing an annual report on key policy and media questions.
“Our observational, statistical, and modeling tools for assessing and projecting fire are improving rapidly, but the problem of extreme fires always remains one step ahead of us,” says Douglas Kelley, fire scientist at the UK Centre for Ecology & Hydrology (UKCEH). “To catch up, we need our tools to provide quick, robust answers to critical questions about climate impact, human causation, affected communities, and future risks. These answers need to be communicated clearly to non-specialists when they are most needed.”
The third priority aims to explore how fires affect marginalized and underrepresented communities, emphasizing Indigenous populations and environmental justice.
“So how should we be using all the tools at our disposal to improve measurements and help create better models for predicting the downstream effects of each fire?” Hamilton asks. “And once we do that, how do we best communicate these findings to our communities? We wanted to create a roadmap for science, so that our collaborations focus on getting these answers faster than at present.”
A main goal in the white paper is to be able to improve fire modeling, predictability, and mitigation on both regional and global scales, but Hamilton also hopes that FLARE will aid in fostering transdisciplinary science and in recruiting future fire scientists. “There simply are not enough scientists in this field to do the work,” Hamilton says.
Sebastian Diez from Universidad del Desarrollo, Chile and part of International Global Atmospheric Chemistry’s (IGAC) Early Career Committee further emphasizes the importance of global collaboration. “Researchers from the Global South face unique challenges that require locally adapted solutions,” Diez says. “Strengthening research capabilities and resources in less affluent regions is imperative to effectively address the transdisciplinary challenges of fire science.”
“Fire has always been there in the Earth System, what’s new is how it is being affected by and affecting humans in the context of wider planetary change,” says Sophie Hebden, Future Earth. By bringing together the different global research networks of Future Earth we were able to address these challenges across research silos and outline a transdisciplinary research agenda for the global fire community,” says Sophie Hebden, research coordinator with Future Earth.
As fire events become more intense and frequent, the urgency for effective and proactive fire science grows. FLARE’s next steps are to address these challenges collectively, as a unified fire research community, to better protect our planet and its inhabitants.
The workshop was supported by global research networks including the Surface Ocean Lower Atmosphere Study (SOLAS), International Global Atmospheric Chemistry (IGAC), and Past Global Changes (PAGES) as well as organizations including European Space Agency (ESA), National Aeronautics and Space Administration (NASA), Met Office UK, and Centre for Ecology & Hydrology (CEH). The working group is funded by the ESA-Future Earth joint program. The workshop was further supported by NC State University, PAGES, and the Bermuda Institute of Ocean Sciences (BIOS).
The white paper, “Igniting Progress: Outcomes from the FLARE workshop and three challenges for the future of transdisciplinary fire science,” is open access, and available here .
- Designing Healthy and Resilient Societies
- college of sciences
- marine earth and atmospheric sciences
- the abstract
More From NC State News

Bartonella and Babesia Co-Infection Detected in Patients with Chronic Illness

Apparel Industry Leaks Millions of Tons of Plastic Into Environment Each Year, Study Finds

AI Powers Interdisciplinary Innovation
Ed Research Isn’t Always Relevant. This Official Is Trying to Change That

- Share article
Classroom apps, tools, and programs, many driven by artificial intelligence, evolve faster than quality control efforts can keep up.
This more tech-driven and interconnected education landscape will require a different approach to research, development, and evaluation, according to the head of the U.S. Education Department’s research agency.
Matthew Soldner, the acting director of the Institute of Education Sciences, called for a faster and more robust “research and development ecosystem” to build structures to ensure new programs and tools are effective in the classroom.
For example, while IES traditionally awards grants for five-year studies, it has launched one new pilot called “Seedlings to Scale,” in which cohorts of research teams will compete for three rounds of progressively larger grants: first to create a prototype and indicators of success; next to develop the program or product and test its effectiveness; and finally to take successful programs to scale. Only about a quarter of the initial cohort will make it to full scale.
Soldner spoke with Education Week about how he sees education research changing. This interview has been edited for length and clarity.
How do you see technology changing the focus of education research?
Particularly when the product is educational technology, the pace of development just so rapidly outstrips not just the capacity of the [What Works Clearinghouse] but the capacity of traditional forms of impact research.
Look, for example, at the frequency with which districts change textbook adoptions, the textbook is changing every three or four years. It barely provides time for that textbook to get into the classroom, to have some sort of rigorous study done, and have the results looked at before it changes again, where that version of the product is no longer commercially available, and the publisher moves on to the next. The pace is nearly impossible to do the depth of research you might like, and so we have to continue to find models that will allow us to be responsive to that.
You’ve expressed interest in a “living evidence” model. How does that differ from the current research models?
The principle is that we should always be searching the literature to find the latest research on a topic, incorporating that new research into our understanding of what works, and giving that information out to our public as quickly as possible.
You might think that’s how everything operates currently, but actually, it’s not. If we want to, for example, work on struggling adolescent literacy, we will survey all the literature in that space, do our publication, and then not monitor that literature for a period of time until we decide to come back to that topic. [If] something is published, then let’s say 20 or 25 years go by, and people begin to wonder how things changed.
In many areas, the literature is changing so quickly, so dramatically that you would need to be updating a practice guide every two or three years. But at least you would be monitoring that literature ... and people would have confidence that you had in fact looked at the most recent research. It’s a real fundamental shift, in terms of this constant monitoring of the flow of incoming evidence.
How is IES’s new push for R&D scale-up different from prior initiatives?
It is thought to be a pipeline, a continuous [movement] upward in evidence building. In terms of scale, we really are getting a wealth of aligned investments around a shared topic, really investing time and energy in those. ... It’s a bit more structured, it’s a bit more hands on, with the expectation that if you are showing that your project is a good fit to what the market is looking for and is effective, that you will have the opportunity to move up.
It’s our intention that this really places the educator and the classroom at the center of the development effort in that first phase.
IES has made science education one of those priority areas. Why focus on science now?
Science [education] really is a space where perhaps even less is known than math, or at least we have less rigorous evidence about what works and we have the same kind of real dire performance gaps. If we look back at the data that we have from 2019, more than 40 percent of all 12th graders were below basic [in the National Assessment of Educational Progress for science]. And that’s so much worse for Hispanic students—about half—and Black students, about 70 percent. So that science proficiency gap is huge.
As a nation, we have chosen to make more and larger investments in the nation’s long-term competitiveness and our national security than ever before in [science, technology, engineering, and math]. That includes AI, clean energy, pandemic preparedness ... but if we’re going to realize that moment and, and turn those dollars into progress, we have to have increasing levels of science and math literacy amongst our students.
The pandemic massively disrupted education research. How much have we been able to recover that research capacity?
I think we are still in [the] throes of recovering from the pandemic. In some places, schools aren’t yet ready to return to having researchers on the ground or research being conducted in schools the way they once were. Recruitment, even for new studies, continues to be a challenge.
We have been talking with any group of researchers who will listen on ways in which researchers can think about really engaging communities with the work they’ve proposed to do. We’re suggesting strongly that researchers spend a lot of time on the ground with schools they are trying to recruit, trying to understand what problems they are trying to solve, … [and] making sure that the research is truly responsive to their needs.
Where do you see the biggest potential for paradigm-shifting research in education?
It is more often the case that folks want to understand basic pedagogy or test that in an intervention, than that they are bringing entirely new models of how we might structure teaching and learning. So, what if learning took place in a system or in a model that was very different from what we have today? What if the systems we have today were better connected and more seamlessly bridged education systems with social support systems?
I think if we’re looking for true paradigm shifts, it’s likely to be less some new intervention, some new ed tech product, but instead something that really disrupts how teaching and learning is delivered.
Sign Up for EdWeek Update
Edweek top school jobs.

Sign Up & Sign In

New research helps unlock the secrets of flow, an important tool for creative and problem solving tasks
Does it seem like everyone's talking about 'flow', all of a sudden?
Maybe because many people are. Flow has been shown to help those experiencing it become effortlessly absorbed in a creative or problem-solving task, and more resistant to distraction, whether that task be writing, playing sport, conducting surgery or making music.
New research is routinely emerging extolling the virtues of the seemingly-elusive mental state, and its enormous potential for creativity and performance.
A recent study out of Drexel University's Creative Research Lab in Philadelphia, led by Dr. John Kounios, sought to examine the 'neural and psychological correlates of flow' in a sample of jazz guitarists.
Some guitarists were very experienced and some less so, with the study looking at what their brains were up to while they improvised.
Study participants were fitted with EEG (electroencephalogram) electrode caps and their brain activity was monitored while performing an improvisation to a pre-determined chord progression, or jazz 'lead'.
They were then told to self-report their experience of flow. Their performances were subsequently assessed for quality by a panel of musical experts.
According to the study, the participants with the most experience found their flow most easily and also gave the best-rated performances. This was found to be from a combination of established skills and their capacity to 'let go.'
Similarly, the EEGs of the best-performing improvisers showed reduced activity in the superior frontal gyri of their brains. This region is associated with executive control, or conscious decision-making.
Letting go, in this instance, means a relinquishing of conscious control.
What is flow, and how can it help us
Mihalyi Csikszentmihalyi was the psychologist who first identified flow: "a state in which people are so involved in an activity that nothing else seems to matter; the experience is so enjoyable that people will continue to do it even at great cost, for the sheer sake of doing it."
ABC Classic presenter and registered psychologist Greta Bradman breaks down the flow state further:
"Being in flow feels good. You might not even have a sense of time when doing a task, be it washing the dishes or getting into a gnarly work task.
"There's this real sense of having focus or meeting the world in flow."
For people working in highly competitive fields where optimised performance is vital, like music performance, being able to tap into tools like flow can make a huge difference for success.
Dr. Steffen Herff, leader of the Sydney Music, Mind and Body Lab at Sydney University, suggests one way flow might help musicians find that cutting edge.
"One component that makes flow so interesting from a cognitive neuroscience and psychology perspective, is that it comes with a 'loss of self-consciousness'," he says.
The fears and insecurities that come with performing to an audience are pushed from the forefront of the mind.
"In other words, gone are all these pesky thoughts of self-doubt."
The benefits of flow for peak creativity
Herff and his team are continually exploring ways to best support musicians both mentally and physically, with techniques such as biofeedback and mental imagery.
Herff says improvising requires a lot of split-second decisions, alongside high-level creative judgements.
By introducing flow into this process, "all the fears, desires, and anxieties that hold you back are gone, whilst at the same time [you're] able to draw more efficiently from all the hours of practise and experience you have accumulated over the years."
Pianist, composer and improviser Nat Bartsch first heard about flow in her Honours year at the Victorian College of the Arts.
As an artist with autism and ADHD, Bartsch has learnt to deliberately foster ways of creating time and space to find that flow state.
"What I love about this study is that it dispels the myth that artists must always wait for 'inspiration to strike' – to be a professional artist is to be able to switch your creativity on and off, on any given day."
She agrees that experience makes all the difference, particularly when it comes to letting go.
"If you know who you are on the stage, or at your instrument, it's easier to let go and trust in what you'll come up with."
Finding flow by letting go
The study's authors explain that flow requires three conditions: "a balance between challenge and skill, clear, proximate goals, and immediate feedback about progress and performance."
It makes sense, then, that a more experienced player would be able to access these conditions more readily. They've had more time to develop skills, set directions for themselves, and form the capacity to critically analyse their own work. And then, let that go.
While flow is not the only way to develop one's musical improvisation skills, Herff acknowledges that this new research is exciting in showing great potential in helping to clarify the brain processes that determine whether a flow state is achieved.
Kounios is clear that practice makes perfect, but flow is about letting go, leaving those looking to find it with one last piece of advice taken from jazz great Charlie Parker:
"You've got to learn your instrument. Then, you practise, practise, practise. And then, when you finally get up there on the bandstand, forget all that and just wail."
Sign up to the ABC Classic Newsletter
- X (formerly Twitter)
Related Stories
You can use music to change your mood — but there's a catch.
Hitting the high notes: The rich history of jazz at the ABC
There wasn't a jazz club when James Valentine was growing up in Ballarat. Instead he tuned into the ABC
What happened when a concert pianist wore a heart rate monitor during a marathon performance
- Neuroscience
- The University of Sydney
- United States
The trends defining the $1.8 trillion global wellness market in 2024
From cold plunges to collagen to celery juice, the $1.8 trillion global consumer wellness market is no stranger to fads, which can sometimes surface with limited clinical research or credibility. Today, consumers are no longer simply trying out these wellness trends and hoping for the best, but rather asking, “What does the science say?”
About the authors
This article is a collaborative effort by Shaun Callaghan , Hayley Doner, Jonathan Medalsy, Anna Pione , and Warren Teichner , representing views from McKinsey’s Consumer Packaged Goods and Private Equity & Principal Investors Practices.
McKinsey’s latest Future of Wellness research—which surveyed more than 5,000 consumers across China, the United Kingdom, and the United States—examines the trends shaping the consumer wellness landscape. In this article, we pair these findings with a look at seven wellness subsets—including women’s health, weight management, and in-person fitness—that our research suggests are especially ripe areas for innovation and investment activity.
The science- and data-backed future of wellness
In the United States alone, we estimate that the wellness market has reached $480 billion, growing at 5 to 10 percent per year. Eighty-two percent of US consumers now consider wellness a top or important priority in their everyday lives, which is similar to what consumers in the United Kingdom and China report (73 percent and 87 percent, respectively).
This is especially true among Gen Z and millennial consumers, who are now purchasing more wellness products and services than older generations, across the same dimensions we outlined in our previous research : health, sleep, nutrition, fitness, appearance, and mindfulness (Exhibit 1). 1 “ Still feeling good: The US wellness market continues to boom ,” McKinsey, September 19, 2022.
Across the globe, responses to our survey questions revealed a common theme about consumer expectations: consumers want effective, data-driven, science-backed health and wellness solutions (Exhibit 2).
Five trends shaping the consumer health and wellness space in 2024
Fifty-eight percent of US respondents to our survey said they are prioritizing wellness more now than they did a year ago. The following five trends encompass their newly emerging priorities, as well as those that are consistent with our earlier research.

Trend one: Health at home
The COVID-19 pandemic made at-home testing kits a household item. As the pandemic has moved into its endemic phase, consumers are expressing greater interest in other kinds of at-home kits: 26 percent of US consumers are interested in testing for vitamin and mineral deficiencies at home, 24 percent for cold and flu symptoms, and 23 percent for cholesterol levels.
At-home diagnostic tests are appealing to consumers because they offer greater convenience than going to a doctor’s office, quick results, and the ability to test frequently. In China, 35 percent of consumers reported that they had even replaced some in-person healthcare appointments with at-home diagnostic tests—a higher share than in the United States or the United Kingdom.
Although there is growing interest in the space, some consumers express hesitancy. In the United States and the United Kingdom, top barriers to adoption include the preference to see a doctor in person, a perceived lack of need, and price; in China, test accuracy is a concern for approximately 30 percent of consumers.
Implications for companies: Companies can address three critical considerations to help ensure success in this category. First, companies will want to determine the right price value equation for at-home diagnostic kits since cost still presents a major barrier for many consumers today. Second, companies should consider creating consumer feedback loops, encouraging users to take action based on their test results and then test again to assess the impact of those interventions. Third, companies that help consumers understand their test results—either through the use of generative AI to help analyze and deliver personalized results, or through integration with telehealth services—could develop a competitive advantage.
Trend two: A new era for biomonitoring and wearables
Roughly half of all consumers we surveyed have purchased a fitness wearable at some point in time. While wearable devices such as watches have been popular for years, new modalities powered by breakthrough technologies have ushered in a new era for biomonitoring and wearable devices.
Wearable biometric rings, for example, are now equipped with sensors that provide consumers with insights about their sleep quality through paired mobile apps. Continuous glucose monitors, which can be applied to the back of the user’s arm, provide insights about the user’s blood sugar levels, which may then be interpreted by a nutritionist who can offer personalized health guidance.
Roughly one-third of surveyed wearable users said they use their devices more often than they did last year, and more than 75 percent of all surveyed consumers indicated an openness to using a wearable in the future. We expect the use of wearable devices to continue to grow, particularly as companies track a wider range of health indicators.
Implications for companies: While there is a range of effective wearable solutions on the market today for fitness and sleep, there are fewer for nutrition, weight management, and mindfulness, presenting an opportunity for companies to fill these gaps.
Wearables makers and health product and services providers in areas such as nutrition, fitness, and sleep can explore partnerships that try to make the data collected through wearable devices actionable, which could drive greater behavioral change among consumers. One example: a consumer interested in managing stress levels might wear a device that tracks spikes in cortisol. Companies could then use this data to make personalized recommendations for products related to wellness, fitness, and mindfulness exercises.
Businesses must keep data privacy and clarity of insights top of mind. Roughly 30 percent of China, UK, and US consumers are open to using a wearable device only if the data is shared exclusively with them. Additionally, requiring too much manual data input or sharing overly complicated insights could diminish the user experience. Ensuring that data collection is transparent and that insights are simple to understand and targeted to consumers’ specific health goals or risk factors will be crucial to attracting potential consumers.
Trend three: Personalization’s gen AI boost
Nearly one in five US consumers and one in three US millennials prefer personalized products and services. While the preference for personalized wellness products was lower than in years prior, we believe this is likely due to consumers becoming more selective about which personalized products and services they use.
Technological advancements and the rise of first-party data are giving personalization a new edge. Approximately 20 percent of consumers in the United Kingdom and the United States and 30 percent in China look for personalized products and services that use biometric data to provide recommendations. There is an opportunity to pair these tools with gen AI to unlock greater precision and customization. In fact, gen AI has already made its way to the wearables and app space: some wearables use gen AI to design customized workouts for users based on their fitness data.
Implications for companies: Companies that offer software-based health and wellness services to consumers are uniquely positioned to incorporate gen AI into their personalization offerings. Other businesses could explore partnerships with companies that use gen AI to create personalized wellness recommendations.
Trend four: Clinical over clean
Last year, we saw consumers begin to shift away from wellness products with clean or natural ingredients to those with clinically proven ingredients. Today, that shift is even more evident. Roughly half of UK and US consumers reported clinical effectiveness as a top purchasing factor, while only about 20 percent reported the same for natural or clean ingredients. This trend is most pronounced in categories such as over-the-counter medications and vitamins and supplements (Exhibit 3).
In China, consumers expressed roughly equal overall preference for clinical and clean products, although there were some variations between categories. They prioritized clinical efficacy for digestive medication, topical treatments, and eye care products, while they preferred natural and clean ingredients for supplements, superfoods, and personal-care products.
Implications for companies: To meet consumer demand for clinically proven products, some brands will be able to emphasize existing products in their portfolios, while other businesses may have to rethink product formulations and strategy. While wellness companies that have built a brand around clean or natural products—particularly those with a dedicated customer base—may not want to pivot away from their existing value proposition, they can seek out third-party certifications to help substantiate their claims and reach more consumers.
Companies can boost the clinical credibility of their products by using clinically tested ingredients, running third-party research studies on their products, securing recommendations from healthcare providers and scientists, and building a medical board that weighs in on product development.
Trend five: The rise of the doctor recommendation
The proliferation of influencer marketing in the consumer space has created new sources of wellness information—with varying degrees of credibility. As consumers look to avoid “healthwashing” (that is, deceptive marketing that positions a product as healthier than it really is), healthcare provider recommendations are important once again.
Doctor recommendations are the third-highest-ranked source of influence on consumer health and wellness purchase decisions in the United States (Exhibit 4). Consumers said they are most influenced by doctors’ recommendations when seeking care related to mindfulness, sleep, and overall health (which includes the use of vitamins, over-the-counter medications, and personal- and home-care products).
Implications for companies: Brands need to consider which messages and which messengers are most likely to resonate with their consumers. We have found that a company selling products related to mindfulness may want to use predominately doctor recommendations and social media advertising, whereas a company selling fitness products may want to leverage recommendations from friends and family, as well as endorsements from personal trainers.
Seven areas of growth in the wellness space
Building upon last year’s research, several pockets of growth in the wellness space are emerging. Increasing consumer interest, technological breakthroughs, product innovation, and an increase in chronic illnesses have catalyzed growth in these areas.
Women’s health
Historically, women’s health has been underserved and underfunded . Today, purchases of women’s health products are on the rise across a range of care needs (Exhibit 5). While the highest percentage of respondents said they purchased menstrual-care and sexual-health products, consumers said they spent the most on menopause and pregnancy-related products in the past year.
Digital tools are also becoming more prevalent in the women’s health landscape. For example, wearable devices can track a user’s physiological signals to identify peak fertility windows.
Despite recent growth in the women’s health space, there is still unmet demand for products and services. Menopause has been a particularly overlooked segment of the market: only 5 percent of FemTech start-ups address menopause needs. 2 Christine Hall, “Why more startups and VCs are finally pursuing the menopause market: ‘$600B is not “niche,”’” Crunchbase, January 21, 2021. Consumers also continue to engage with offerings across the women’s health space, including menstrual and intimate care, fertility support, pregnancy and motherhood products, and women-focused healthcare centers, presenting opportunities for companies to expand products and services in these areas.
Healthy aging
Demand for products and services that support healthy aging and longevity is on the rise, propelled by a shift toward preventive medicine, the growth of health technology (such as telemedicine and digital-health monitoring), and advances in research on antiaging products.
Roughly 70 percent of consumers in the United Kingdom and the United States and 85 percent in China indicated that they have purchased more in this category in the past year than in prior years.
More than 60 percent of consumers surveyed considered it “very” or “extremely” important to purchase products or services that help with healthy aging and longevity. Roughly 70 percent of consumers in the United Kingdom and the United States and 85 percent in China indicated that they have purchased more in this category in the past year than in prior years. These results were similar across age groups, suggesting that the push toward healthy aging is spurred both by younger generations seeking preventive solutions and older generations seeking to improve their longevity. As populations across developed economies continue to age (one in six people in the world will be aged 60 or older by 2030 3 “Ageing and health,” World Health Organization, October 1, 2022. ), we expect there to be an even greater focus globally on healthy aging.
To succeed in this market, companies can take a holistic approach to healthy-aging solutions , which includes considerations about mental health and social factors. Bringing products and services to market that anticipate the needs of aging consumers—instead of emphasizing the aging process to sell these products—will be particularly important. For example, a service that addresses aging in older adults might focus on one aspect of longevity, such as fitness or nutrition, rather than the process of aging itself.
Weight management
Weight management is top of mind for consumers in the United States, where nearly one in three adults struggles with obesity 4 Obesity fact sheet 508 , US Centers for Disease Control and Prevention, July 2022. ; 60 percent of US consumers in our survey said they are currently trying to lose weight.
While exercise is by far the most reported weight management intervention in our survey, more than 50 percent of US consumers considered prescription medication, including glucagon-like peptide-1 (GLP-1) drugs, to be a “very effective” intervention. Prescription medication is perceived differently elsewhere: less than 30 percent of UK and China consumers considered weight loss drugs to be very effective.
Given the recency of the GLP-1 weight loss trend, it is too early to understand how it will affect the broader consumer health and wellness market. Companies should continue to monitor the space as further data emerges on adoption rates and impact across categories.
In-person fitness
Fitness has shifted from a casual interest to a priority for many consumers: around 50 percent of US gym-goers said that fitness is a core part of their identity (Exhibit 6). This trend is even stronger among younger consumers—56 percent of US Gen Z consumers surveyed considered fitness a “very high priority” (compared with 40 percent of overall US consumers).
In-person fitness classes and personal training are the top two areas where consumers expect to spend more on fitness. Consumers expect to maintain their spending on fitness club memberships and fitness apps.
The challenge for fitness businesses will be to retain consumers among an ever-increasing suite of choices. Offering best-in-class facilities, convenient locations and hours, and loyalty and referral programs are table stakes. Building strong communities and offering experiences such as retreats, as well as services such as nutritional coaching and personalized workout plans (potentially enabled by gen AI), can help top players evolve their value proposition and manage customer acquisition costs.
More than 80 percent of consumers in China, the United Kingdom, and the United States consider gut health to be important, and over 50 percent anticipate making it a higher priority in the next two to three years.
One-third of US consumers, one-third of UK consumers, and half of Chinese consumers said they wish there were more products in the market to support their gut health.
While probiotic supplements are the most frequently used gut health products in China and the United States, UK consumers opt for probiotic-rich foods such as kimchi, kombucha, or yogurt, as well as over-the-counter medications. About one-third of US consumers, one-third of UK consumers, and half of Chinese consumers said they wish there were more products in the market to support their gut health. At-home microbiome testing and personalized nutrition are two areas where companies can build on the growing interest in this segment.
Sexual health
The expanded cultural conversation about sexuality, improvements in sexual education, and growing support for female sexual-health challenges (such as low libido, vaginal dryness, and pain during intercourse) have all contributed to the growth in demand for sexual-health products.
Eighty-seven percent of US consumers reported having spent the same or more on sexual-health products in the past year than in the year prior, and they said they purchased personal lubricants, contraceptives, and adult toys most frequently.
While more businesses began to sell sexual-health products online during the height of the COVID-19 pandemic, a range of retailers—from traditional pharmacies to beauty retailers to department stores—are now adding more sexual-health brands and items to their store shelves. 5 Keerthi Vedantam, “Why more sexual wellness startups are turned on by retail,” Crunchbase, November 15, 2022. This creates marketing and distribution opportunities for disruptor brands to reach new audiences and increase scale.
Despite consistently ranking as the second-highest health and wellness priority for consumers, sleep is also the area where consumers said they have the most unmet needs. In our previous report, 37 percent of US consumers expressed a desire for additional sleep and mindfulness products and services, such as those that address cognitive functioning, stress, and anxiety management. In the year since, little has changed. One of the major challenges in improving sleep is the sheer number of factors that can affect a good night’s sleep, including diet, exercise, caffeination, screen time, stress, and other lifestyle factors. As a result, few, if any, tech players and emerging brands in the sleep space have been able to create a compelling ecosystem to improve consumer sleep holistically. Leveraging consumer data to address specific pain points more effectively—including inducing sleep, minimizing sleep interruptions, easing wakefulness, and improving sleep quality—presents an opportunity for companies.
As consumers take more control over their health outcomes, they are looking for data-backed, accessible products and services that empower them to do so. Companies that can help consumers make sense of this data and deliver solutions that are personalized, relevant, and rooted in science will be best positioned to succeed.
Shaun Callaghan is a partner in McKinsey’s New Jersey office; Hayley Doner is a consultant in the Paris office; and Jonathan Medalsy is an associate partner in the New York office, where Anna Pione is a partner and Warren Teichner is a senior partner.
The authors wish to thank Celina Bade, Cherry Chen, Eric Falardeau, Lily Fu, Eric He, Sara Hudson, Charlotte Lucas, Maria Neely, Olga Ostromecka, Akshay Rao, Michael Rix, and Alex Sanford for their contributions to this article.
This article was edited by Alexandra Mondalek, an editor in the New York office.
Explore a career with us
Related articles.

Still feeling good: The US wellness market continues to boom

How to thrive in the global wellness market

Feeling good: The future of the $1.5 trillion wellness market

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- J Crit Care Med (Targu Mures)
- v.4(1); 2018 Jan
The Importance of Referencing
Ario santini.
1 University of Medicine and Pharmacy of Tîrgu Mureș, Tîrgu Mureș, Romania
2 Hon Fellow, University of Edinburgh, Edinburgh, United Kingdom
It is imperative that authors of medical papers give fitting credit to the sources that they quote in their manuscripts. Frequently this is not the case, and a wrong, inappropriate or unsuitable citation often blights the quality of a paper. Many concerns can proceed from questions relating to improper citations. These matters may be directed at a personal level or may have a bearing on the general research community. They can range from doubt being levied at the individual’s academic ability, to his/her academic honesty, or even the suggestion of potential plagiarism. Meticulous referencing of sources will eliminate all of these concerns.
The stamp of a good research worker is attention to detail at all levels of his/her research. Attention to detail cultivates good habits and the detail required in referencing and preparing a bibliography focuses attention on the whole research procedure. It aids scientific thought and analysis and makes for better research reporting.
Good referencing includes attention to detail such as correct page numbering, the spelling of author’s names and the accuracy of relevant facts that will be stated in the paper. Attention to referencing not only makes you a better researcher but enhances your reputation amongst editors, reviewers and readers.
An editor or reader may interpret poor referencing as a sign of intellectual laziness, unclear thinking, and inaccurate writing. When you cite sources correctly, you leave no question in your readers’ minds regarding your point. By citing precisely and accurately, the phrase “It is said” need ever be used in your academic manuscript.An excellent bibliography shows off your scientific knowledge. An extensive bibliography is the hallmark of a widely read and well-informed clinician or scientist.
Errors of omission frequently are the cause of a reviewer not accepting a manuscript for publication. By not citing a critical or well-known paper extant in the scientific literature, authors can be accused of not having undertaken an extensive literature review or having inadequate knowledge of their subject. It may even lead a reviewer to consider that the work is, in part, plagiarised.
Reviewers look at the bibliography for several reasons. Attention to detail, with regard to spelling and punctuation, as stated above, is a primary concern. Moreover, the citation method, be it Harvard or Vancouver or other, must strictly follow the instructions to authors as prescribed by the journal in question. If the most recent reference is more than five years or so, this may indicate that a full up to date review of the literature has not been undertaken. A preponderance of references by one author(s) may suggest self- promotion, self- plagiarism, or the selective citation of papers whose conclusion are in accord with those of the author.
Plagiarism is a prominent problem encountered in the academic process and is one of the most common causes of compromising the academic integrity of the author. Sources must be cited in an appropriate form. Copying, using, or the misuse of other people’s ideas, words or concepts, without proper referencing is prohibited. It is not enough to change a few words in a phrase from the source material into “own words”. Changing the word-order of a sentence is unacceptable, as is the use of synonyms. Referencing and references, signify the quality of the work, detail the primary sources and are indicative of the extent of information on the subject. Proper referencing removes any question of plagiarism.
Every submitted academic manuscript is scrutinised several times before it is accepted for publication. The process starts with editors, progresses via reviewers and continues even after acceptance when editorial assistants will locate sources in the bibliography and ensure that the citations are accurate.
Your manuscript is much more likely to survive the rigours of the review process with minimal criticism and positive feedback if all references are contemporaneous, refer to a primary source and have been accurately and correctly cited.
Additional Reading
- Share full article
Advertisement
Supported by
Concerned About Metals in Tampons? Here’s What to Know.
A recent study detected a number of metals in many types of tampons. Experts weigh in on the findings and what they could mean for your health.

By Dana G. Smith and Katie Mogg
A new study about tampons has sparked concern among consumers. The research, published in the journal Environment International, found evidence of 16 different metals in a wide range of tampons sold in the United States and Europe.
In the days since news of the study came out, women have taken to social media to express their alarm about the findings. “Soo nice of them to let us know they found LEAD & ARSENIC in our tampons 20 years after I started my period,” one TikTok user posted .
But while these findings can sound scary, several experts, including one of the scientists who led the research, said they are not a reason to panic, nor to immediately stop using tampons.
Levels of the toxic chemicals detected, including arsenic and lead, were very low, and two prior studies by the same group of researchers did not find significantly higher blood levels of the metals in women who use tampons compared with those who don’t.
“There’s small amounts of these metals found, really, everywhere,” said Dr. Bethany Samuelson Bannow, an associate professor of medicine specializing in hematology at Oregon Health and Science University, who was not involved in the study. “I would actually be less concerned about having these metals in tampons than I would about having them in food or water.”
Here’s what to know about the research and what it might mean for your health.
What the study found
The researchers analyzed 30 tampons from 14 different brands for arsenic, barium, calcium, cadmium, cobalt, chromium, copper, iron, manganese, mercury, nickel, lead, selenium, strontium, vanadium and zinc.
We are having trouble retrieving the article content.
Please enable JavaScript in your browser settings.
Thank you for your patience while we verify access. If you are in Reader mode please exit and log into your Times account, or subscribe for all of The Times.
Thank you for your patience while we verify access.
Already a subscriber? Log in .
Want all of The Times? Subscribe .
We're sorry but you will need to enable Javascript to access all of the features of this site.
Stanford Online
Cybersecurity: why it matters now.

From ransomware to state-sponsored hacks, Stanford’s Neil Daswani explains why cybersecurity is more relevant than ever.
Though it may be hard for many of us to remember life before the internet, it was only in the the early 90s that U.S. Vice President Al Gore coined the term “information superhighway” to describe a then new technology that allowed us to connect, share information, and do business at previously unimaginable speeds.
And just as it did for the cars-and-asphalt highways that preceded it, it is taking decades to figure out how to make the information superhighway safe for users.
“When horseless carriages started getting peak deployment in the 1920s, there were a lot of accidents. It was not until 1958 that Volvo first designed the lap and shoulder seat belt. It wasn't until 10 years after that that the federal government required that such seat belts were installed in call vehicles except busses,” explains Neil Daswani, Co-Director of the Stanford Advanced CybersecurityProgram, Chief Information Security Officer at QuantumScape, and co-author of Big Breaches: Cybersecurity Lessons for Everyone and Foundations of Security: What Every Programmer Needs to Know. “The internet got commercialized in the mid-90s. We are still in a golden age of cybersecurity advancement.”
With much work remaining to be done to secure our IT systems, Daswani explained in a recent webinar, “Breaking and Entering: How to Get a Cybersecurity Job,” we need cybersecurity professionals now more than ever.
20,000 discovered breaches per year / 20,000 breaches over 20 years
While cybersecurity has come a long way in 30 years, there are still plenty of reasons to be concerned for the safety of your data. According to Daswani, experts identify over 20,000 new vulnerabilities in our information systems every year and log them into the national vulnerabilities database. A vulnerability can be a starting point for a breach, and in the past 20 years, America has been the victim of over 20,000 cybersecurity breaches.
“Effectively, every time that you view a web page, you could be exposing yourself in one or more ways. I think we definitely need to get to a better state in the world,” insists Daswani.
The Covid-19 pandemic only increased the need for robust cybersecurity by accelerating the adoption of remote work. According to the U.S. census, the number of Americans working from home tripled between 2019 and 2021. While many have since returned to the office or are working from home only part-time, it remains true that more people are now using personal devices and unsecured networks for work, increasing their vulnerability to cyber attacks.
The Internet is convenient, but it can be a dangerous place. According to a 2022 report by Radware, 95% of organizations currently use at least one form of cloud services. Yet 70% are not confident about their cybersecurity. Which makes sense given 69% of organizations suffered a recent data breach and more than half face application attacks once a month or more.
A matter of national security
It is not only personal data and companies that are under threat. So too are governments. American information systems are increasingly vulnerable to attacks by third parties, often working for foreign governments.
Daswani considers the impact of such recent attacks in Big Breaches. In one case study, he shows how the December 2020 hacking of SolarWinds, a company with 300,000 customers, gave the Russians a backdoor into the U.S. Departments of Justice, Commerce, and Treasury. The WannaCry attack, launched by the North Koreans in 2017, infected over 200,000 machines across the world, including those at hospitals and universities. The effects of such attacks can be costly. Cybersecurity Ventures estimates the global cost of cybercrime will reach $8 trillion in 2023 .
Daswani is clear: “The threat of cyber war is increasing. Power grids have been targeted. Ransomware was responsible for disrupting an oil pipeline for an entire week before a ransom was paid.”
He is far from the only one highlighting this mounting threat. It has been barely two years since President Joe Biden issued an executive order telling all federal agencies that they need to take steps to secure themselves and all their suppliers.
Work that makes a difference
Despite these alarming stories and statistics, the size of the threat translates to huge opportunity for workers interested in working in the field. Whether you are looking for entry-level employment, pivoting from an adjacent field, or seeking to advance your existing career, now is the ideal time to explore a career in cybersecurity.
Cyberseek.org reports over 600,000 current job openings in cybersecurity within the United States. Out of those 600,000 job openings, 130,000 or more are for cybersecurity analysts–an entry-level position attracting former IT systems administrators and network engineers, amongst others. The US Bureau of Labor Statistics estimates the number of information security analyst positions will grow by 31%, much faster than the 4% national average across professions. According to the Bureau of Labor Statistics, the mean annual wage for Information Security Analysts is just under $120,000.
Cybersecurity is not just a field that is in-demand and lucrative, it is also a field where you can make a real difference.
As Robert Rodriguez, chairman and founder of cybersecurity organization SINET, explains in his advance reaction for Big Breaches, “what makes this profession different from most other jobs is the opportunity to have a sense of purpose and mission. Professionals in this business are, in their own small way, an essential part of the higher calling toward the protection of their respective nation’s critical infrastructures, their national and economic security, privacy, and inherent rights as free citizens in a free democracy.”
If you are energized by the idea of working on the digital frontlines to protect personal, corporate, and national data, you can start with introductory courses in information security, such as Stanford Online’s Foundations of Information Security . Those looking for comprehensive training led by top industry professionals can explore the variety of resources available to you and your team at Stanford Online .
- Engineering
- Computer Science & Security
- Business & Management
- Energy & Sustainability
- Data Science
- Medicine & Health
- Explore All
- Technical Support
- Master’s Application FAQs
- Master’s Student FAQs
- Master's Tuition & Fees
- Grades & Policies
- Graduate Application FAQs
- Graduate Student FAQs
- Graduate Tuition & Fees
- Community Standards Review Process
- Academic Calendar
- Exams & Homework FAQs
- Enrollment FAQs
- Tuition, Fees, & Payments
- Custom & Executive Programs
- Free Online Courses
- Free Content Library
- School of Engineering
- Graduate School of Education
- Stanford Doerr School of Sustainability
- School of Humanities & Sciences
- Stanford Human Centered Artificial Intelligence (HAI)
- Graduate School of Business
- Stanford Law School
- School of Medicine
- Learning Collaborations
- Stanford Credentials
- What is a digital credential?
- Grades and Units Information
- Our Community
- Get Course Updates
COMMENTS
Research investment has responded to this, and other health challenges in recent years. For example, there has been a significant move towards greater collaboration between researchers, nurses, patients and family caregivers to address the needs identified as important by the community.
As Research entails testing, verifying, and rejecting hypotheses regularly, keeping up with recent publications will assist you in defining building blocks for your study. Guidance & Confirming that your Research is focused on a new topic. One of the key responsibilities for a doctorate adviser, department head, or field expertise is to advise ...
A working knowledge of research - both how it is done, and how it can be used - is important for everyone involved in direct patient care and the planning & delivery of eye programmes. The mention of 'research' can be off-putting and may seem irrelevant in the busy environment of a clinic or hospital. However, research is central to all ...
Here are some important reasons why you should be up-to-date with all the latest publications in your field: 1. To identify a novel research topic and future research opportunities. Understanding the current status of knowledge on a particular topic, identifying gaps, and zeroing in on a question that is relevant and answerable are the initial ...
Peer Review is defined as "a process of subjecting an author's scholarly work, research or ideas to the scrutiny of others who are experts in the same field" ( 1 ). Peer review is intended to serve two primary purposes. Firstly, it acts as a filter to ensure that only high quality research is published, especially in reputable journals ...
Placing research in the bigger context of its field and where it fits into the scientific process can help people better understand and interpret new findings as they emerge. A single study usually uncovers only a piece of a larger puzzle. Questions about how the world works are often investigated on many different levels.
1. Introduction. This article is part of a series describing evidence-based research—the use of prior research in a systematic and transparent way to inform a new study so that it is answering questions that matter in a valid, efficient, and accessible manner [1].By prior research, we mean original studies (also called primary studies), but even when planning a new systematic review ...
In this first article of a three-article series, we introduce the evidence-based research approach. Evidence-based research is the use of prior research in a systematic and transparent way to inform a new study so that it is answering questions that matter in a valid, efficient, and accessible manner.
In this, the first of three articles, we aim to define and describe evidence-based research. We introduce here, and in the subsequent articles provide more details for, the use of an evidence-based research approach before embarking on new research to justify and design the new study (article #2 in series) and, after the completion of the study, to place its results of the new study in the ...
NOTABLE RESEARCHERS. Psychological research has a long history involving important figures from diverse backgrounds. While the introductory chapter discussed several researchers who made significant contributions to the discipline, there are many more individuals who deserve attention in considering how psychology has advanced as a science through their work ().
All being said, do we exactly know how old a research article can be before it gets the label of not being recent i.e., an old article not good for citing. There is consensus among scientists and researchers that articles less than five years old are recent publications. However, it may vary from discipline to discipline.
A recent United Kingdom report on the use of personal data in health research concluded that public involvement in research is necessary for the success of information-based research, and that a public informed about the value of research is likely to have greater enthusiasm and confidence in research and the research community . Moreover ...
Some archival data sets offer important insights but are not updated to the recent past. For example, the U.S. census is updated every 10 years. A scholar asking a research question requiring census data for an answer might be forced to use data up to 10 years old. A second example is the Pew religious data, which are updated every 7 years.
For example, if you cite sources from the current century as well as 1930s, then a paper from 2010 should be considered recent, but not one from 1950. If, on the other hand, your temporal range of references is rather narrow, say, recent 20 years, then you should refer to as "recent" for sources that are from approximately last 4-5 years.
Strength in research helps to define a university's "brand" in the national and international marketplace, impacting everything from student recruitment, to faculty retention, to attracting ...
a calls-for-papers service.BooksBooks will be of more use i. some research areas than others. A few databases include books but the best way to keep up to date is t. rough the publishers' websites. The major academic publishers, as listed under 'Journal issues' above, offer this, but also check the websites of publishers who specialise in ...
A few weeks ago, when submitting an abstract to a nursing conference, I was suddenly faced with a dilemma about age. Not my own age, but the age of evidence I was using to support my work. One key element of the submission criteria was to provide five research citations to support the abstract, and all citations were to be less than ten years old.
Seminal research articles and/or foundational books can remain relevant for a long time and help establish the context for a given paper. ... if you are submitting an article to a journal in a fast-developing field like neuroscience, more recent sources—if relevant and important for your readers to consider in the context of your paper ...
1.2 Why research is important. The UK is a world leader for research and invention in healthcare, with around 25% of the world's top 100 prescription medicines being discovered and developed in the UK (The impact of collaboration: The value of UK medical research to EU science and health). Research in the health and care system is important ...
In order to support evidence-based policy making, timeliness of research is important. Methods. Examples are provided, e.g. where research was on time to be included in the policy process and where research was too late to be included in it. These examples are described and analysed to provide for recommendations on how to better align both ...
An up-to-date systematic review is important for researchers to decide whether to embark on new research or continue supporting ongoing studies. The aim of this study is to examine the time taken between the last search, submission, acceptance and publication dates of systematic reviews published in nursing journals. Nursing journals indexed in Journal Citation Reports were first identified.
Hello Kenn - Welcome to the forum! A review of related - and preferably recent - literature is meant to set your research in the context of what is currently known about the topic and to establish that what you have to offer is novel, something different from what has been already attempted.The review also reassures the referees that you are familiar with current developments in your ...
cept of critical inquiry. Research grows out of the primary human tendency or need to learn, to know, to solve problems, to question received wisdom and take. -for-granted assumptions. These impulses are fundamentally critical; the need to know is the counterpoint to the sense that what is already know.
A new white paper on the many ways wildfires affect people and the planet makes clear that as fires become more intense and frequent, the urgency for effective and proactive fire science grows. By addressing these challenges, the fire research community aims to better protect our planet and its inhabitants. Fire is a natural part of life on Earth, sustaining healthy and balanced ecosystems ...
For example, while IES traditionally awards grants for five-year studies, it has launched one new pilot called "Seedlings to Scale," in which cohorts of research teams will compete for three ...
A recent study out of Drexel University's Creative Research Lab in Philadelphia, led by Dr. John Kounios, sought to examine the 'neural and psychological correlates of flow' in a sample of jazz ...
Despite recent growth in the women's health space, there is still unmet demand for products and services. Menopause has been a particularly overlooked segment of the market: only 5 percent of FemTech start-ups address menopause needs. 2 Christine Hall, "Why more startups and VCs are finally pursuing the menopause market: '$600B is not ...
The stamp of a good research worker is attention to detail at all levels of his/her research. Attention to detail cultivates good habits and the detail required in referencing and preparing a bibliography focuses attention on the whole research procedure. ... If the most recent reference is more than five years or so, this may indicate that a ...
A recent study detected a number of metals in many types of tampons. Experts weigh in on the findings and what they could mean for your health. By Dana G. Smith and Katie Mogg A new study about ...
Discover why cybersecurity is more crucial than ever in our digital age. Stanford's Neil Daswani explores the increasing threats and the urgent need for cybersecurity professionals. ... Which makes sense given 69% of organizations suffered a recent data breach and more than half face application attacks once a month or more. A matter of ...